China Stands (Almost) Alone: Zero-COVID Lessons for America and the World
China’s management of COVID-19 has been an outstanding success. For the entire course of the pandemic, China has identified 100,386 cases as of December 19, 2021, of which 80,000 occurred prior to March 2020. In a population of 1.4 billion, over a period of 21 months since March of 2020, there have been about 20,000 confirmed cases. For the entire course of the pandemic to date, China has recorded 4,636 deaths, nearly all of which occurred prior to May 2020 during the initial outbreak in Wuhan.
This success has been sustained through the delta and now the omicron variants. The peak of new cases after the arrival of the delta variant in China was 113 on August 10, 2021. Cases declined thereafter. Since the arrival of omicron, cases have plateaued in the eighties per day during December [1].
Moreover, “Sustained containment has high socioeconomic value: economic activities recovered rapidly [after the initial outbreak], with an increase in gross domestic product of 3.2% during April through June 2020, and of 4.9% during July through September 2020; the government’s response to the pandemic was perceived positively by the Chinese public” [39].
In contrast, the United States has suffered over 50 million confirmed cases in a population that is a quarter of China’s. And with the arrival of omicron, daily new cases are over 130,000 and climbing steeply. Over 800,000 people have died; over 1,000 are now dying each day [2]. Forecasts for the coming months have become dire [136].
The economic impact of the pandemic has also been in stark contrast to China’s experience. For calendar 2020, China’s economy grew at a 2.3% rate while the U.S. economy shrank 3.4% [45]. China’s was the only major economy to experience growth in 2020.

The remainder of this essay considers whether we should learn from China’s pandemic response, if so what, and lastly whether we are capable of doing so. The following sections are constructed as follows:
- Blaming China: two versions, examines how China has been blamed for the coronavirus in order to appreciate why its strategy for containing and suppressing COVID has been widely ignored.
- Is China’s success real or a product of manipulated data? considers another factor standing in the way of learning from China’s response, the suspicion that China’s data on the numbers of COVID cases and deaths is underreported.
- Origins and initial outbreak first looks at efforts to find the source of SARS-CoV-2 and the debate over whether it originated zoonotically or from a laboratory incident. It then closely examines the circumstances of the initial outbreak and the role of local government officials in concealing its seriousness.
- China’s response to the COVID-19 crisis: coordination, mobilization, and containment examines the major features of China’s successful “zero-COVID” policy.
- Conclusions summarizes the elements of China’s zero-COVID policy and, in closing, considers to what extent the United States — and other countries — are capable of learning from it.
1. Blaming China: two versions
China’s success has been overshadowed by criticisms of its mismanagement of the initial outbreak. The more public, and very effective, version of this has cultivated an association of COVID with China (the “Wuhan virus”); blamed China as the source of the outbreak, either via a “lab leak” or because of dangerous social practices (consumption of wild meat); accused the Chinese government of knowingly concealing the outbreak; and demanded reparations from it. A parallel set of criticisms among researchers and pundits has traced the alleged mismanagement to China’s authoritarian government.
1.1 The Trump Administration’s public attacks
The public campaign of vilification began at a March 22, 2020 press conference, when then President Trump
accused Beijing of concealing the outbreak first detected in Wuhan that has become a pandemic now paralyzing the United States. “Certainly, the world is paying a big price for what they did,” he said. And the next day, he was joined at a White House briefing by Secretary of State Mike Pompeo, who accused China’s government of distorting vital health data and said its response “creates risk to people all around the world” [144].
This came after an initial period, from January until early March, when the Trump administration sought to downplay the seriousness of COVID and overstate the effectiveness of the U.S. response [147].
Trump and other administration officials continued to use “Chinese virus”, “Wuhan virus”, and even “kung flu” for months in an effort to fix blame for the pandemic on China [145, 146].
1.2 Pandemic mismanagement as a consequence of authoritarian government
Authoritarian governments, it is argued, may be adroit at mobilization and coordination in response to crises, but they are prone to suppressing warning signals that, had they been heeded, would prevent many crises from occurring in the first place or at least would reduce their impact. More pithily, “Autocracy impedes uncovering emerging problems” [60]. As Yuen Yuen Ang put in his summary of this dilemma:
Strong authoritarian regimes excel at mass mobilization, but to prevent epidemics from arising in the first place, a government requires ‘democratic characteristics’ — that is, a climate that empowers not only civil society but also public officials to speak candidly about problems without fear of reprisals. Conversely, having a democracy by itself is no guarantee of efficacy; it must also be combined with wise leadership and state capacity [19].
1.3 An assessment of criticisms of China’s pandemic response
The Trump administration pivoted from rosy reassurances about COVID to attacks on China when it became apparent that, due in part to its own management failures, the virus would have a severe impact on American society and the economy in an election year. This alone would be reason to suspect that the attacks were an effort to scapegoat and shift attention. In addition, though, it has since come to light that Trump had already been informed of the seriousness of COVID by his own national security staff and directly by China’s President, Xi Jinping.
On January 28, his national security advisor, Robert O’Brian, told the President unequivocally that COVID “will be the biggest national security threat you face in your presidency”. And on February 6 the Chinese President informed Trump in a phone call that the coronavirus was transmissible through air and could be up to five times as deadly as the flu. He also alerted Trump to the extraordinary measures China was taking to contain it [148].
What, though, of the claim that China’s authoritarian government was responsible? There are reasons be cautious about such a critique.
- As shown in detail below, the period during which the local — not national — government concealed information about the outbreak was no more than three weeks. That the national government was not responsible for concealing the outbreak was subsequently confirmed by U.S. intelligence agencies, who concluded that officials in Beijing “were kept in the dark for weeks about the potential devastation of the virus by local officials in central China” [143].
- It is not self-evident that the problem of reporting “bad news” is specific to authoritarian governments. And when, in mid-January, the national government did realize the seriousness of the problem, it responded with extraordinary clarity, thoroughness, and forcefulness.
- Lastly, if the problem is framed as a need to know immediately when there are signs of a disease outbreak, then there is reason to believe that authoritarian governments could become effective at this, because it is a matter of the right instructions and incentives. It is only when the problem is framed as ‘What space exists in civil society or in the ground-level institutional system to raise alarms about unexpected threats?’ that authoritarian governments may be more vulnerable to failure.
SARS-CoV2 is not a “Chinese” virus, but a virus that first appeared in China. The next pandemic could start almost anywhere. The 1918 flu epidemic, for example, probably originated in North America (it was misnamed the “Spanish flu”) [149]. What’s needed is to strengthen international systems for monitoring and controlling epidemic diseases.
2 Is China’s success real or a product of manipulated data?
But is China’s success an illusion cultivated through under-reporting of cases and denial of access to researchers? There are multiple sources of evidence that the initial outbreak in Wuhan and the province of Hubei was worse than officially acknowledged or, more likely, realized, by the Chinese government. One group of researchers used China’s Disease Surveillance Point (DSP) system to show that the total mortality rate in Wuhan was 56% higher than expected in the first quarter of 2020 [3]. And a major study by the Chinese Center for Disease Control and Prevention (CDC) of COVID antibody levels found that 4.43% of Wuhan residents had contracted COVID. In a city of 11,000,000, this is about 473,000 people, far more than the 50,354 confirmed cases of COVID-19 reported by officials [4, 5].
However, the primary failing of local government lay not in undercounting cases as the epidemic raged, but in suppressing information about it during a key three-week period from December 30, 2019 — when it was informed by reliable sources of evidence of a SARS-like disease spreading — until January 20, 2020, when the National Health Commission confirmed human-to-human transmission of a novel coronavirus.
The larger picture these and other studies paint is that the 76-day lockdown of Wuhan, along with other containment measures initiated and coordinated through the State Council’s Joint Prevention and Control Mechanism, were successful [137]. The DSP system study noted that “no increase in overall mortality was found during the three months of the covid-19 outbreak in other parts of China”. And the Chinese CDC study found that only 0.44% of people living in Hubei province outside Wuhan had antibodies, and less than 0.1% of those in six other provinces included in the study had them. Additional evidence that COVID reporting subsequent to the initial outbreak has been accurate and, if anything, unusually thorough is provided in a review by Donna Lu in New Scientist [26]. A mass screening that tested almost the entire adult population of Wuhan between May 14 and June 1, 2020 found “no newly confirmed COVID-19 cases, and identified 300 asymptomatic positive cases” (this is discussed in more detail below) [46].
More generally, China has implemented among the most thorough epidemiological surveillance and screening systems in the world to support its “zero COVID” policy [25, 39], without which this policy could not have been achieved or sustained.
The assessment that China has succeeded in containing the virus, and that case data subsequent to March 2020 is accurate, is supported by the fact that Chinese society, and the Chinese economy, have been able to largely return to normal. By August of 2020, a reporter for the New York Times noted that
In Shanghai, restaurants and bars in many neighborhoods are teeming with crowds. In Beijing, thousands of students are heading back to campus for the fall semester. In Wuhan, where the coronavirus emerged eight months ago, water parks and night markets are packed elbow to elbow, buzzing like before [7].
In September, “in-person learning [was offered] for about 195 million students in kindergarten through 12th grade at public schools” [8].
Holiday travel also recovered: “In just the first week of October 2020, about 637 million Chinese were travelling during the Golden Week holidays, not far behind the pre-pandemic equivalent of 782 million in 2019” [9].
And as noted earlier, the Chinese economy, despite shrinking 6.8% in the first quarter of 2020, grew 2.3% for the year, the only major economy to achieve growth in 2020 [10, 11].
Nothing viscerally conveys the thoroughness of China’s suppression of COVID better than the massive pool party held in Wuhan in August:
Given the total lockdown of Wuhan to suppress the virus, it is highly unlikely that this event would have been permitted were there any danger of a super-spreader event.
3 Origins and initial outbreak
The origins of COVID-19, referred to as SARS-CoV-2 [12], remain obscure. A study of the earliest confirmed cases found that the onset of symptoms in the earliest patient was December 1, 2019 [47]. An analysis combining epidemiological and phylogenetic methods estimated that SARS-CoV-2 probably emerged between mid-October and mid-November 2019. This analysis did not shed light on the ultimate source of the virus but did distance the index case from the outbreak at the Huanan Seafood Wholesale Market [48].
It was not until December 31 that the Wuhan CDC reported a cluster of unknown pneumonia cases believed to be related to the Huanan Seafood Wholesale Market. The market was closed the next day from concern that a virus had been transmitted to humans from an intermediate host animal there [13, 14].
Despite an extensive investigation by the World Health Organization and others, there remain several plausible theories about the source of the disease. SARS-CoV-2's close genetic similarity to multiple previously identified bat coronaviruses supports a zoonotic origin. However, some of the earliest cases do not appear connected to the seafood market, and there is circumstantial evidence for the possibility of a laboratory incident at the Wuhan Institute of Virology, which has performed SARS research since 2005. The Chinese government has so far refused to permit an investigation of this. A recent reanalysis in Science by Michael Worobey, a leading expert in tracing the evolution of viruses, shows that the first case could have been a seafood vendor at the Huanan Market, but there is insufficient data to consider this conclusive [138, 139].
An assessment, by the National Intelligence Council, shows that intelligence agencies are uncertain of SARS-CoV-2’s origin and would not be able to provide “a more definitive explanation … unless new information allows them to determine the specific pathway for initial natural contact with an animal or to determine that a laboratory in Wuhan was handling SARS-CoV-2 or a close progenitor virus before COVID-19 emerged” [20]. The report concluded that
China’s officials probably did not have foreknowledge that SARS-CoV-2 existed before WIV [Wuhan Institute of Virology] researchers isolated it after public recognition of the virus in the general population. Accordingly, if the pandemic originated from a laboratory-associated incident, they probably were unaware in the initial months that such an incident had occurred [20].
The search for the source of SARS-CoV-2 points to the accelerating dissolution of conceptual and physical boundaries between humanity and nature. On the one hand, diminished habitats are increasingly interwoven with human settlements. In a recent study, scientists built a model analyzing how frequently coronaviruses might spill over from bats to people across southern China and southeast Asia. By overlaying the habitats of bats known to harbor SARS-related coronaviruses with maps of human populations, they estimated that roughly four hundred thousand people could be infected with SARS-related coronaviruses annually. Spillover is a far more common experience than anyone realizes. “‘These small villages are at the edge of disappearing forests,’ [said] Kendra Phelps, … a co-author on the study. ‘Inside that forest is densely packed wildlife, which is superstressed by things like encroaching palm oil and rice monocultures.’ Stressed animals (just like us) are more likely to get sick and shed virus” [150].
On the other hand, the ability to engineer viruses — and other life forms — is rapidly becoming more sophisticated. In fact, the mRNA vaccines that have been most successful in protecting against COVID are products of viral-vector gene therapies that “use modified viruses as drug-delivery vehicles to introduce specific DNA sequences — encoding genes, regulatory RNAs … or other therapeutic substrates — into cells” [151]. Even if SARS-CoV-2 was the result of a laboratory incident, the global reality is that laboratory biosafety regulation and monitoring is not what it needs to be virtually anywhere.
In a review of biosafety and biosecurity published shortly before the pandemic, the authors wrote that the “world has become more integrated and now shares a common destiny in terms of biosafety. In the face of the current risks and challenges, the international community must work together to avert threats, advance mutual interests, and safeguard global biosecurity” [152; see also 15, 16, 20]. The present pandemic only accentuates this need and must inspire stronger common action rather than deepen divisions.
3.1 Local government response
The local government’s initial response blended denial and repression. Despite growing evidence of human-to-human transmission it first dismissed, then downplayed this possibility through most of January, including concealing some cases from the CCDC (Chinese Center for Disease Control and Prevention). It summoned several doctors who had spoken-up about early cases to the police and warned them not to be “spreading misinformation.” It did virtually nothing to alert the people of Wuhan to the threat, and the Kitchen God Festival, an annual potluck in which over 40,000 families participated, was allowed to be celebrated on January 19 [13].
As noted, the Chinese government’s authoritarianism is often held responsible for the local government’s failures. A careful analysis by Yu Liu and Richard Saltman of local government decision-making in the critical period between late December — when compelling evidence of an outbreak emerged — and late January — when the national government assumed overall control of crisis management [49] — illustrates how structural decision biases, along with a congeries of unfortunately timed events, led the local government to suppress information about the outbreak and mislead national authorities [22].
Liu and Saltman emphasize that local government’s key responsibilities are “economic development and the preservation of social stability”. Pursuant to this, officials would not want Lunar New Year celebrations January 24–30 to be disrupted, or for that matter the prestigious provincial-level meeting of the All-China People’s Congresses and Political Consultative Conferences that were scheduled in Wuhan January 12–17. The likelihood that officials were led to “underestimate the potential hazard of the emerging epidemic” was exacerbated by several additional factors. First, national expert health teams were strictly confined to a technical advisory role. They were only supposed to provide input to local leaders. Second, the early police admonishment of doctors who’d warned of a SARs-like outbreak had the effect of silencing medical staff as they became aware of human-to-human transmission. And lastly, none of the top officials in Wuhan or Hubei province had a medical or public health background [22].
When community transmission began in January, the city of Wuhan was unprepared. The outbreak “exposed the weak capacity of community hospitals, including outdated equipment, low competency of doctors, as well as limited ability for virus testing and monitoring”. Many patients, not trusting these institutions, went instead to large hospitals, leading to cross-infection. The number of healthcare workers were insufficient to cope with the “tremendous influx of patients with COVID-19”. Soon, there was a “dire shortage of personal protective equipment (PPE) for healthcare workers”, further increasing the risk of infection. As the outbreak expanded to other locations, shortages of “ventilators, gloves, surgical masks, disposable isolation gowns, eye protection, essential medicines, and equipment” were widely reported [18].

4 China’s response to the COVID-19 crisis: coordination, mobilization, and containment
4.1 Fundamental Principles
At the outset of the national government’s response, it articulated a set of principles intended to orient and guide what would quickly become an immense mobilization and containment effort:
- The outbreak “must be given high priority and all efforts should be made to prevent and control the disease.”
- “put the safety of people’s lives and health first, formulate careful plans, organize all parties to carry out prevention and control, take effective measures and resolutely curb the spread of the epidemic.
- “make every effort to treat patients, as soon as possible to identify the causes of viral infection and transmission, strengthen case surveillance.”
- “release information in a timely manner and deepen international cooperation.”
- Departments and localities should “implement early detection, early reporting, early isolation, early treatment and centralized treatment measures” [27].
In sum, “solidarity and the paramountcy of life” are core values, and protecting health and ensuring public health security are key goals [21].
In addition, on January 23 China raised its national public health response to the highest state of emergency: Level 1 of 4 levels of severity in the Chinese Emergency System, defined as an “extremely serious incident” [29].
The decisiveness of China’s response may have stemmed in part from prior experience. “Late in 2002, China suffered from a SARS outbreak, one of the contagious coronaviruses that resulted in 8,098 infections and 774 deaths from 32 countries. Although SARS was effectively contained, preparations of China and other countries were insufficient for the epidemic at that time in terms of late reporting to health officials, inadequate quarantine and isolation measures, poor hygiene precautions, and vulnerability of healthcare workers” [30].
4.2 Joint Multi-Sectoral Cooperation
The next day, January 24, a Joint Prevention and Control Mechanism of the State Council was established involving 32 Ministries, with sub-groups on control of outbreak, medical rescue, scientific research, information and communication, international cooperation, logistics, and frontline coordination [21, 28].
4.3 Stopping Transmission — Emergency Control Measures
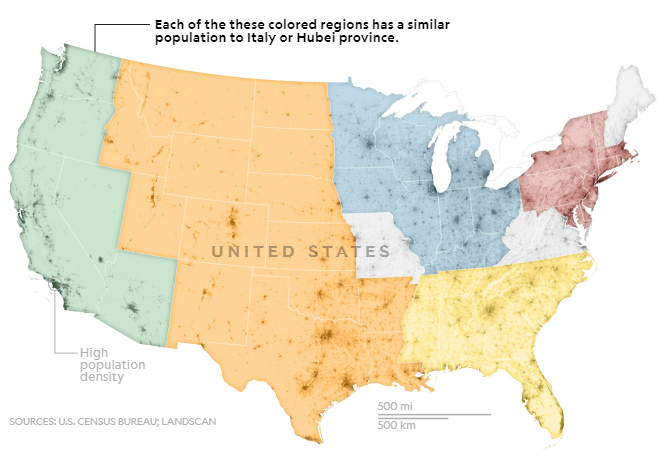
To prevent further dispersal of COVID-19 from its source, all transport was prohibited in and out of Wuhan city from 10:00 AM on 23 January 2020, followed by the whole of Hubei Province a day later. In terms of the population covered, this appears to be the largest attempted cordon sanitaire in human history. Some idea of the magnitude — nearly 60 million people — is suggested by this illustration (Italy is mentioned because it imposed a national lockdown on March 9, 2020) [31]:
During the lockdown, which in Wuhan lasted until April 8, all public transport by bus and subway rail was suspended, schools and entertainment venues were closed, public gatherings were banned, and health checks were carried out on migrants (“floating population”). All non-essential companies, including manufacturing plants, were shut down [29].
In some areas, “closed management” was implemented on a community basis. This typically meant that villages, communities, and units would only keep one entrance and exit point open, and each household was allowed limited numbers of entrances and exits. In some places, night-time access was prohibited, effectively a curfew, and in extreme cases, access was prohibited throughout the day. People entering and leaving were required to wear masks and receive temperature tests [32, 133].
In all, emergency control measures were implemented in 342 cities across China. School closure, the isolation of suspected and confirmed patients, plus the disclosure of information were implemented in all cities. Public gatherings were banned and entertainment venues closed in 220 cities (64.3%). Intracity public transport was suspended in 136 cities (39.7%), and intercity travel was prohibited by 219 cities (64.0%). All three measures were applied in 136 cities [29].
Many of these same measures were implemented in rural areas, including prohibitions of movement into and out of villages and of public gatherings [58].
Social distancing and outside mask wearing were universally mandated.
In addition, all “incoming international travelers, workers handling imported goods, medical-center outpatients with fever or respiratory symptoms, and medical staff caring for patients with fever or infectious diseases are actively screened with PCR to determine if they are infected. Incoming travelers have been required to quarantine at designated hotels for 14 days after entry into China, during which time they are tested at least twice” [39].
To provide adequate care in Wuhan in the face of a caseload that escalated rapidly until late February, when there were over 65,000 cumulative confirmed cases [33], the National Health Commission (NHC) mobilized 42,600 multidisciplinary medical workers and 965 public health workers from other provinces to support Hubei. Over 11,000 doctors and nurses with expertise in critical care (almost 10 percent of China’s critical care workers) were sent to Wuhan [21, 34, 44].
4.3.1 In-patient Quarantine and Hospital Expansion
In Wuhan, officials decided against home isolation for mild to moderate cases, as home isolation is not always properly complied with, and it was difficult to organize medical care and monitoring for those in isolation. Furthermore, home isolation could be psychologically taxing on the patients as patients know they are putting family members at risk of infection [35].
As an alternative, a tiered system of in-patient care was organized. This was a mammoth and unprecedented undertaking. The bottom tier consisted of Fangcang hospitals. As Simiao Chen and her collaborators explain,
Fangcang shelter hospitals were developed and used for the first time in China to tackle the coronavirus disease 2019 (COVID-19) outbreak. The term Fangcang, which sounds similar to Noah’s Ark in Chinese, was borrowed from military field hospitals, but it refers to a novel concept: large, temporary hospitals built by converting public venues, such as stadiums and exhibition centres, into health-care facilities to isolate patients with mild to moderate symptoms of an infectious disease from their families and communities, while providing medical care, disease monitoring, food, shelter, and social activities [36].
Total capacity in 16 Fangcang hospitals reached 13,348 beds by February 21, after which the need for beds began declining [37, 42]. The first three Fangcang hospitals added 4000 beds and were prepared in 29 hours [36]. The first hospital closed on March 1, 2020; by March 10, all Fangcang shelter hospitals had been suspended.

For more severe cases, patients “were gathered for treatment and intensive care at the best hospitals with the greatest capacity for accommodating patients with infectious respiratory diseases [42]. Two hospitals, Huoshenshan and Leishenshan, with a combined a capacity of 2,500 beds, were built in the space of two weeks, with the second hospital opening on February 7th [38, 42]. As a result of these and other measures, the “number of beds for severe cases quickly increased from around 1,000 to more than 9,100” [42].
3.4 Testing
Early in the epidemic testing capacity was inadequate, leading to delayed diagnosis and treatment [40]. To mitigate this, Hubei “adjusted diagnostic criteria to include clinical diagnosed cases as a compliment for the count of new confirmed cases aimed at accelerating the identification and treatment of patients”, according to the journalist Zhao Hong. The iterations of the Diagnosis and Treatment Protocols for Patients with Novel Coronavirus Pneumonia show these variations in diagnostic criteria [41].
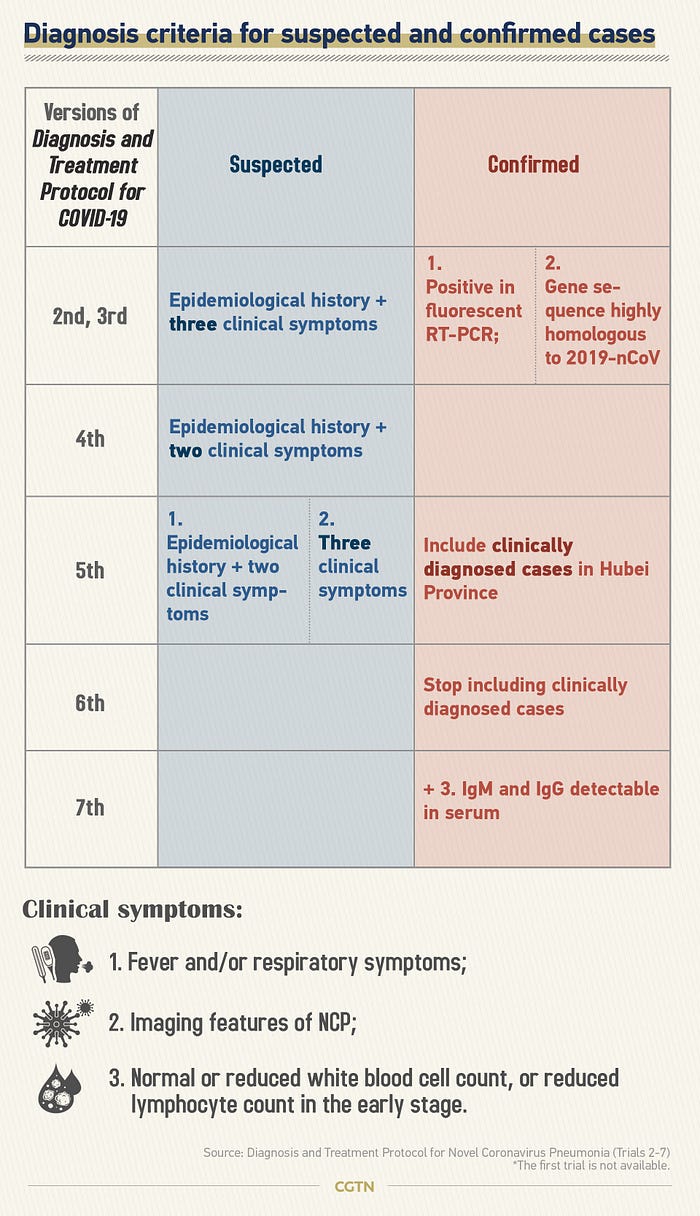
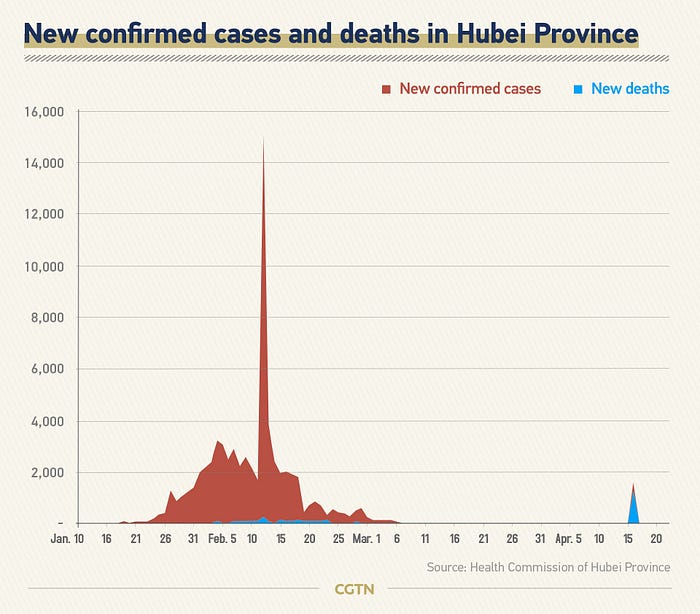
The brief period when cases were counted as confirmed with only clinical symptoms and no PCR or antibody tests generated the huge spike in cases reported on February 13, as noted in the timeline and shown below [43].
China rapidly scaled-up its capacity to produce, distribute, analyze, and report on COVID tests. Some of the key milestones in this effort were included in a white paper the State Council published in June of 2020 [42]:
- January 10: Research institutions including China CDC and the Wuhan Institute of Virology (WIV) under the Chinese Academy of Sciences (CAS) came up with an initial version of test kits.
- February 15: seven types of test reagents had been approved for market launch.
- April 1: Chinese customs began nucleic acid testing (NAT) on inbound arrivals at all points of entry — air, water and land.
- by mid-April: In Hubei Province, the testing period was shortened from 2 days to 4–6 hours, and the daily capacity expanded from 300 samples in the early stage of the epidemic to more than 50,000 in mid-April. Such advances made early detection and confirmation of infection possible and reduced the risk of transmission.
The last point alludes to the fact that testing became very extensive for all groups considered at higher risk, as already noted. In addition, “once a local outbreak is identified, geographic jurisdictions are classified by epidemiologists into regions at low, moderate or high risk of transmitting the virus. People in high-risk settings are tested individually. In moderate-risk areas, a 5:1 or 10:1 pooled sampling approach is used to reduce the number of tests” [39].
Ultimately, two mass screenings were conducted in Wuhan. The first is poorly documented but probably consisted of screening people as they returned to work, as noted in a Wall Street Journal article from mid-April 2020: “Nucleic-acid tests are now mandatory for anyone leaving the city, and while they aren’t compulsory for those returning to work, many companies are demanding them. Some employers also require antibody tests. Several hospitals have started doing both for all patients and staff” [51]. Industries began resuming operations in Wuhan from March 21 [57].
The second mass screening, between May 14 and June 1, became globally famous due its scale, coordination, and rapidity. As summarized by Shiyi Cao and her collaborators in a follow-up study of the results,
There were 10,652,513 eligible people aged ≥6 years in Wuhan (94.1% of the total population). The nucleic acid screening was completed in 19 days (from May 14, 2020 to Jun 1, 2020), and tested a total of 9,899,828 persons from the 10,652,513 eligible people (participation rate, 92.9%). Of the 9,899,828 participants, 9,865,404 had no previous diagnosis of COVID-19, and 34,424 were recovered COVID-19 patients. The screening … found no newly confirmed COVID-19 cases, and identified 300 asymptomatic positive cases with a detection rate of 0.303 (95% CI 0.270–0.339)/10,000 [46]. …Of the 34,424 participants with a history of COVID-19, 107 tested positive again, giving a repositive rate of 0.310% (95% CI 0.423–0.574%).
As noted in one account, “Laboratories went from processing around 46,000 tests a day, on average, before the drive, to as many as 1.47 million tests on Friday” [52, 53].
Although Cao et al. asserted that “Virus cultures were negative for all asymptomatic positive and repositive cases, indicating no ‘viable virus’ in positive cases detected in this study”, the implied claim that these 407 asymptomatic cases were not contagious was challenged by other researchers [54] and is contradicted by other studies, including a widely cited analysis that “estimated [using data from a meta-analysis of 8 studies from China] that 59% of transmissions came from individuals who did not present with symptoms (35% presymptomatic; 24% asymptomatic) [55, 56].
This is significant because there were suggestions the Wuhan mass screening effort was unnecessary epidemiologically and was undertaken to reassure the public or as a PR exercise: “public health experts disagree on whether such a resource-intensive push is necessary when infections are low” [52]. In light of the current understanding of asymptomatic transmission, identification and quarantining of the 407 cases may well have been a key step in fully suppressing COVID-19 in Wuhan.
As documented by Zhongjie Li and his co-authors, targeted and mass screenings were used widely in China both preventatively and to quickly shutdown transmission when there were local outbreaks [39].

4.5 Digital Contact Tracing
COVID-19 is mainly transmitted via the respiratory route when people inhale droplets and small airborne particles (that form an aerosol) exhaled by infected people as they breathe, talk, cough, sneeze, or sing. Infected people are more likely to transmit COVID-19 when they are physically close. However, infection can occur over longer distances, particularly indoors. Infectivity can occur 1–3 days before the onset of symptoms. Infected persons can spread the disease even if they are pre-symptomatic or asymptomatic. People are infectious for up to 10 days following symptom onset for persons with mild to moderate COVID-19, and up to 20 days for persons with severe COVID-19 [61]. The danger of aerosol transmission was recognized very early in the pandemic. On February 18, 2020, the Chinese National Health Commission published guidance citing aerosol transmission as a risk [62].
The delta variant, which first appeared in India in late 2020 and has since become the globally predominant form of COVID, is more than twice as contagious as previous variants [63]. The omicron variant that has been spreading since November is still more so [140].
Because COVID is highly contagious, it cannot be fully contained through lockdowns, the use of masks, and social distancing practices. As Philipp Boeing and Yihan Wang note, “The high transmissibility, long incubation period, and existence of asymptomatic patients not only expose the ineffectiveness of traditional mitigation techniques (e.g., wearing masks, keeping physical distance, restricting long-distance travels) but also lead to a rapid exhaustion of public health services” [64].
Contact tracing is a critical public health practice that has been part of epidemic response for centuries. “The traditional way of contact tracing is the manual contact tracing technique, used to identify the close meetups of the infected person. However, the manual contact tracing technique has two significant limitations: (1) it requires a sizeable, trained workforce to conduct these manual interviews; and (2) it cannot identify individuals that are not known to the infected person but have come in close contact (e.g., while using public transport or dining in restaurants). Furthermore, manual contact tracing is a hectic process that requires a centralized, coordinated effort to identify at-risk close contacts of a COVID positive individual” [65].
Digital contact tracing is capable of addressing all of the shortcomings of manual approaches and support full containment of highly infectious diseases. But there are many obstacles to its effective use, as a result of which very few countries have successfully employed it during the COVID pandemic.
“Compared to traditional manual contact tracing constrained by available human resources, scalable digital resources ‘would be sufficient to stop the epidemic if used by enough people, in particular when combined with other measures such as physical distancing.’ By targeting only those citizens at risk, epidemics could be contained without the need for mass quarantines (‘lockdowns’) that are harmful to society in numerous ways” [64].
Digital contact tracing uses smartphone apps to track users’ close contacts. Tracking relies on smartphone location services, which “typically use a combination of cellular, Bluetooth, Wi-fi and the Global Positioning System to determine where people are” to identify all close contacts [65, 77]. When someone is infected with COVID-19 and their positive status is reported in the app, all recent close contacts can be identified, prompting a changed assessment of their risk of contracting COVID. This analysis can be performed in a centralized or distributed mode. “In centralized contact-tracing, the detection is performed in a centralized server. In contrast, in decentralized contact-tracing, each user smartphone acts as a local server that shares only the infected individuals’ data to the centralized server, and then the smartphones will fetch this data periodically from the server and do contact matching locally” [65].

China was the first country to introduce digital contact tracing for COVID, relying on major internet platform companies to do so. On February 9, online payment platform Alipay launched Health Code in Hangzhou in collaboration with the provincial health authority. At almost the same time, messaging and networking platform WeChat introduced its Health Code in the city of Shenzhen. While these two systems are installed on distinct platforms, they have similar functionalities. Subsequently, localized apps implemented in these two platforms have covered more than 500 cities and counties nationwide [66,67].
A key feature of the Health Code apps is that they run as mini programs in WeChat and AliPay, meaning they are present for all users without needing to be downloaded and installed [74]. According to Fan Yang and her collaborators, “Unlike other mini-programs, Health Code programs are automatically added to users’ WeChat and Alipay services, leaving users incapable of deactivating the function, without abandoning the service. This mandatory aspect contributes to the high saturation of the programs across user accounts” [68]. Note, though, that manual registration is still required.
The Health Code apps collect and manage four sets of information:
- Personal data: name, gender, nationality, ID type and number, area of household registration, home address, contact phone number, basic health history, and other information.
- Personal health information: body temperature, current symptoms, information relating to living and staying in high-risk areas, contact with people from high-risk areas, time of health declaration, and other information.
- Travel history: local position for places where the person has recently lived and stayed for a certain period of time, including present location and travel information, and other information.
- Health certification information: assessment result of current health by health information management authorities, including health risk grade assessment, assessment time and reasons for the assessment, medical test results, details of health testing institutions, testing time and sources of data, and other information [69, 70].
Chen and her collaborators [67] note that on February 4, 2020, the Office for Cybersecurity and Information Technology published a notice on the protection of personal information [75]. While this may enhance protection of personal information possessed by tech companies, Rebecca Arcesati, a technology and digital-policy analyst at the Mercator Institute for China Studies in Berlin, cautions that the legal framework treats this data as a strategic resource that belongs to the Chinese state before its citizens [81].
Based primarily on location data in relation to other users, the health code is updated on a daily basis using a three-color scheme to label COVID risk status.
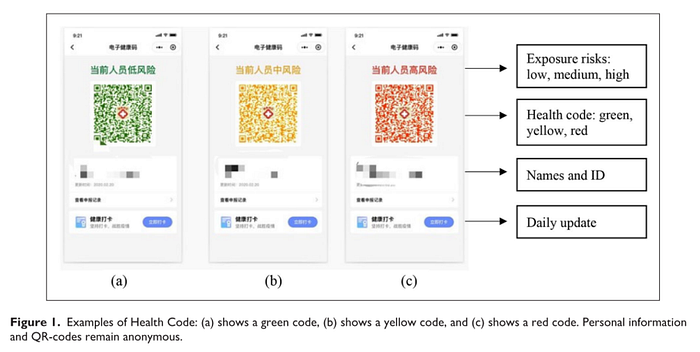
Green allows a person to travel fairly freely. A yellow code indicates that the user should be in home isolation, and red says the user is a confirmed Covid-19 patient and should be in quarantine. People may enter various places such as residential estates and workplaces only when their health code is green [78].
Although use of the Health Code apps is not legally mandated, it is required for movement in public spaces and is thus a practical necessity. WeChat has nearly 1 billion active users in China [66, 71] and AliPay has nearly 700 million [72]. The combination of automatic availability on these platforms and the requirement of use in public spaces means that usage is almost universal. By March of 2021, there were a “total of nearly 900 million” registered users who had collectively used the apps “more than 40 billion person-times” [79]. This is a much higher percentage than the 40–60% threshold required for effectiveness cited in an analysis by Hyunju Kim and Ayan Paul [73]. Only a few other countries, including South Korea and Singapore, have achieved usage sufficient for effective containment.
Although the Health Code apps have had issues with data fragmentation between provinces and code inconsistencies, with some users reporting inexplicable color changes, they have been essential to China’s success in combatting COVID. Their success has depended on the effective use of big data technologies coordinated across many institutions:
The key to the health code is that the verification of data authenticity needs the support of different databases, including the data of confirmed and suspected cases from the National Health Commissions, close contact data from the Ministry of Transport, floating population data from public security, and mobile phone roaming data from telecommunications operators. Data integration and intelligent analysis through the big data platform can be used to distinguish whether an individual is a COVID-19-infected patient, close contact, fellow traveller without close contact, person registered in a fever clinic or person with normal health condition, and finally, two-dimensional health code images with three different possible colours (red, yellow and green) are generated, to divide all of the floating population into three categories [115].
Strong public support also contributes to the success of digital contact tracing in China. A survey by the Mercator Institute found a dramatic contrast between China, on the one hand, and Germany and US, on the other. Support is very high in China, while in Germany and the US there is substantial public opposition. Although survey data from countries with authoritarian governments is subject to distortion, there is a both anecdotal and other survey evidence substantiating public support for the China’s response to COVID, including for contact tracing [76, 132].

Moreover, opposition elsewhere, especially in the US, is exacerbated by the widespread embrace of conspiracy theories. The Mercator survey found that “21 percent of the US respondents and 13 percent of German respondents believe that the Covid-19 pandemic is a conspiracy. This stands in contrast to a mere three percent in China. The survey analysis shows that in all three countries those who share a conspiracy belief are less likely to accept CTAs. This effect is particularly high in the case of the United States, where conspiracy theories like QAnon originated.”
4.5.1 An Example of Digital Contact Tracing with Circle-Layer Management
Much more is involved in containment than apparent in many reports on the use of the Health Code apps. A recent, detailed report by Shan Chen and her collaborators on the management of an outbreak in Chengdu this past summer provides a fuller illustration of a zero-COVID policy in action [80].
The outbreak began on July 27th, when “a family of three in Chengdu were diagnosed as confirmed cases 3 days after their travel to Zhangjiajie, a tourism hotspot that just underwent a clustered outbreak. Another 3 cases were subsequently diagnosed with confirmed infection, including an airport worker, a close contact of the beforementioned family, and a middle-aged female who also traveled to Zhangjiajie several days ago.” Most of the cases involved the Delta variant.
Chengdu promptly implemented a circle-layer quarantine policy that used the Health Code apps to track current risk, supplemented with manual contact tracing. “At the very beginning of the summer outbreak, 29th July, a survey on the epidemiological history of confirmed cases and their close contacts was conducted by workers of corresponding communities and local Center of Disease Control through phone calls, surveillance videos checks, and face-to-face interviews (with personal protective equipment). This information was used to identify the communities and persons at the highest risks of being infected and was uploaded to the Sichuan Big Data Center as the initial information for the circle-layer management and health QR code system.
The circle-layer quarantine policy is a set of risk-level-based containment measures which categorized the potential risk areas into 3 circles or layers: (1) lockdown areas, the areas where the confirmed cases have recently been to; (2) restricted areas, the areas where the close contacts have recently been to; and (3) areas with potential risks, the surrounding areas of the lockdown or restricted areas” [80]. This is illustrated in the infographic below.
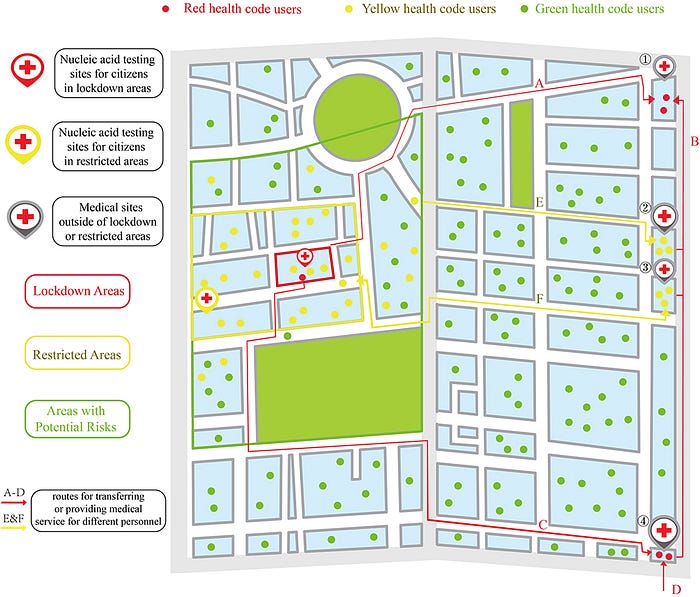
Yellow health codes of users from areas with potential risks turned green once they got a negative nucleic acid testing result, while the red and yellow health codes of users in the lockdown and restricted areas turned green only when they finished quarantine and got negative results in each nucleic acid test.
Circle-layer management in Chengdu ended on August 12th when lockdowns in three communities were lifted, with no new indigenous cases reported for 15 consecutive days. It was successful at suppressing the outbreak, enabling the other 20 million inhabitants of Chengdu to live a normal life without worrying about COVID. As Chen and her collaborators note, success was dependent on the Health Code app, which “timely and precisely collects and updates the COVID-19 correlated symptoms and itinerary information of most citizens, thus enabled governments’ prompt, coherent and accurate decisions on public health policies and the management of citizens with epidemiological history.” Yet they also note many problems, including:
- Code misassignments, especially people receiving yellow or even red codes without apparent justification.
- Burdens imposed on medical facilities due to erroneous red and yellow codes.
- Limitations of care, medical and otherwise, for people with yellow and red codes.
- Lack of transparency about the code algorithm and the distribution, management, and disclosure of personal health data.
- Absence of assurances that data will be protected.
4.5.2 Integrated and Expanded Use of Health Codes
An article in the People’s Daily shows that the government has very ambitious plans for expanding and integrating use of the health code. This is explained through a series of examples:
- East China’s Fujian province has implemented a program that integrates digital health code, medical insurance settlement code, and financial payment code.
- In south China’s Guangdong province, digital health code has helped 70.97 million residents enjoy convenient medical and health services. Each citizen has one health code, and with it the owner can enjoy services at any of the medical and health institutions in the province.
- Hangzhou has integrated citizens’ health code, digital health card and digital social security card, and promoted connectivity and information sharing among relevant institutions and authorities. Such integration is expected to be expanded to more fields in the city such as public transportation, commerce and trade, as well as tourism.
In sum, “‘health code is going to play an increasingly important role in people’s lives’, said Zhou Ping, director of the information technology research center of China Electronics Standardization Institute” [79].
4.6 The Role of Artificial Intelligence in China’s Control of COVID-19
To understand how AI contributed to the management of COVID-19 in China, it helps to be aware of the field’s recent history and the role of the Chinese government and technology industry in promoting and advancing AI research and adoption.
4.6.1 Early 21st Century AI Breakthroughs
The development of AI since the early 1950s has suffered from several “AI winters” stemming from the consequences of inflated expectations and other factors. The most recent of these stretched into the early 2000s and was marked, in part, by researchers using terms such as informatics, machine learning, analytics, knowledge-based systems, business rules management, cognitive systems, intelligent systems, intelligent agents or computational intelligence to avoid the stigma of the term “artificial intelligence” among funders [90].
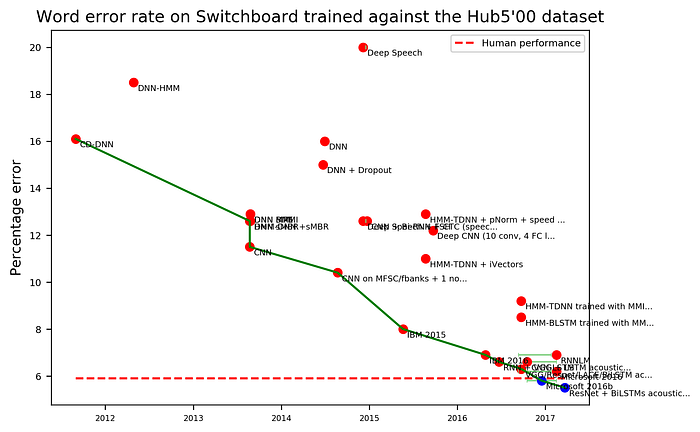
Against this background, a series of breakthroughs using multi-layered neural networks (NNs) were all the more startling. These began in 2012, “when leading researcher Geoffrey Hinton discovered a way to efficiently train those new layers in neural networks” [99]. This resulted in major improvements in speech and visual object recognition, leading to the introduction of voice assistants, auto-transcription and captioning, image searching and cataloging, and many other applications [82, 83, 84]. Additional breakthroughs were followed by further gains in accuracy, in some cases resulting in better than human performance.
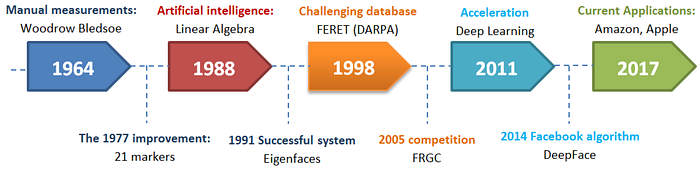
Machine translation was significantly improved using neural machine translation (NMT), with both Google and Microsoft switching to NMT from statistical techniques beginning in 2016 [86, 87]. Face recognition was also accelerated by NNs, with applications that now achieve over 99% accuracy under ideal conditions [88, 89].
4.6.2 Emergence of China’s Artificial Intelligence Strategy
The Chinese government was keenly aware of these and other AI developments, many of which Chinese technology companies were deeply involved in. In fact, Andrew Ng, who left Google in 2014 to become chief scientist at Baidu, has claimed that NMT was “first pioneered and developed and shipped in China” [90].
China has released national-level policy documents promoting AI since 2013 [92, 97]. Its “Internet+” guidance of 2015 was based on the realization that high technologies, mobile Internet, cloud computing, big data, the Internet of Things, and artificial intelligence constituted an industrial revolution. Internet+ was described in terms of a new general-purpose technology [95], with AI one element [93, 94]. In its 5-year plan of 2016, AI was cited as a critical industrial development area.
In 2017, however, there was a major shift in emphasis. With the release of the “New Generation Artificial Intelligence Development Plan” (AIDP), the State Council recognized that “AI has become a new engine of economic development [and the] core driving force for a new round of industrial transformation” [98]. And it set an overall goal that, by 2030
China’s AI theories, technologies, and applications should achieve world-leading levels, making China the world’s primary AI innovation center, achieving visible results in intelligent economy and intelligent society applications, and laying an important foundation for becoming a leading innovation-style nation and an economic power.
Earlier that year, DeepMind’s AlphaGo defeated Ke Jie, the world’s top-ranked Go player, 3–0 in a three-game match [96]. While sometimes cited as a “Sputnik moment” that galvanized China’s AIDP, the timing was likely coincidental [92, 99], though it probably increased support in China for the use of AI [106]. The greater significance of AlphaGo (and its successor, AlphaGo Zero) was in the ascendance of reinforcement learning as an AI methodology [100, 101]. Reinforcement learning “uses algorithms (which often train AI agents or bots) that typically do not rely only on historical data sets, either labeled or unlabeled, to learn to make a prediction or perform a task” [102].
The AIDP undoubtedly advanced AI innovation and use in China, as well as longer-term changes in education and research that will contribute to achieving its goals. China has become a leading hub of AI research and adoption, and by some measures is among the best positioned strategically. A recent Brookings Institution study considered the “number and size of supercomputers in the country as a measure of technological infrastructure, the amount of public and private spending on AI initiatives, the number of AI startups in the country, the number of AI patents and conference papers the country’s scholars produced, and the number of people with STEM backgrounds in the country” in order to characterize the current state and future prospects for AI, based on which China stands-out [103].
4.6.3 The Role of AI in China’s Response to COVID
Artificial intelligence has made contributions to pandemic management in diagnosis, virology and pathogenesis, drug and vaccine development, epidemiology, patient care and outcome, and infodemiology. In many cases, the pandemic has spurred both research and adoption, creating a highly dynamic situation that can be difficult to precisely evaluate, especially with respect to extent and patterns of adoption. It is a situation that leads, frequently, to overly cautious estimates of the rate of change.
The employment of artificial intelligence in China’s response to COVID drew upon a national commitment to AI as an engine of development, along with extensive experience among tech firms and research institutions. In turn, AI’s use in health care has accelerated its overall development and adoption. As François Candelon and his collaborators put it in Fortune:
What stands out isn’t how China is using A.I. to tackle the pandemic, but how deep and specialized its health care data, algorithms, and A.I. research are becoming in the process. Industry-specific vertical innovation is critical for sustained success with A.I., and China’s ability to kick-start that cycle in several industries may enable it to take over the leadership of the global A.I. industry in the not-too-distant future [105].
In reviewing the role of AI in China’s response to COVID, three points stand-out:
- China is playing a leading role globally in AI research related to the pandemic.
- China appears to be among a very few countries to have transitioned some uses of AI into large scale settings within the health care system.
- Data on the extent to which AI technologies are being used is often lacking. And in a few cases, such as the algorithms utilized by the Health Code apps, precise information does not appear to be publicly available.
4.6.3.1 China’s Contributions to AI Research Regarding COVID
Several comprehensive reviews of artificial intelligence research related to COVID have been published recently [107, 108, 109, 110, 111, 112, 113]; most use the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to ensure transparent and complete reporting [107, 109, 110, 111, 113]. Three include data on the country of origin:
- A review of studies of the role of AI in therapeutics for coronavirus disease (drug repurposing, novel drug discovery, and vaccine development) found that more than 50% of all the articles reviewed came from the United States and China (11 and 9 respectively out of 33) [111].
- A review of studies published in English covering the outset of the pandemic (between December 25, 2019, and April 12, 2020), found that 50% were produced in China and 11% in the United States. No other country contributed more than 7% [113].
- In a just published, broad survey of “applications of artificial intelligence for combating the COVID-19 pandemic”, 36% of studies came from China and 19% from the United States. Four countries (China, the United States, India, and Brazil) accounted for nearly three-quarters of the output [112].

These results are consistent with the overall findings of the Artificial Intelligence Index Report for 2021. For 2019, the most recent year for which data was available, 22.4% of all peer-reviewed AI publications were from China, followed by 16.4% from the EU and 14.6% from the United States. Of note, the Report also found that “in 2020, and for the first time, China surpassed the United States in the share of AI journal citations in the world” [114].
4.6.3.2 Two Examples of the Use of Artificial Intelligence in China’s Pandemic Response
Based on need and opportunity, artificial intelligence has been employed in more diverse ways, and to a greater extent, in China than appears to be the case elsewhere. The examples below of AI in diagnosis and in robotics illustrate the complex interplay of public and private research groups, technology corporations, and healthcare institutions with the national government as regulator, sponsor, and, often, envisioning agent. The result appears to be a high degree of innovation ultimately framed and oriented by state guidance and rules.
Diagnosis. When the pandemic struck Wuhan the local health care system was quickly overburdened, and a lack of test kits delayed diagnosis, a situation made worse by the fact that the “early clinical course of SARS-CoV2 infection can be difficult to distinguish from other undifferentiated medical presentations.” Moreover, PCR testing “can take up to 48 hours for operational reasons. Limitations of the gold-standard PCR test for COVID-19 have challenged healthcare systems across the world due to shortages of specialist equipment and operators, relatively low test sensitivity and prolonged turnaround times.” Yet “rapid identification of COVID-19 is important for delivering care, aiding proper triage among patients admitting to hospitals, accelerating proper treatment and minimizing the risk of infection during presentation and waiting hospital admission time” [107].
This led researchers in China and elsewhere to quickly develop AI techniques for diagnosis of COVID-19 from medical imaging (CT scans and chest X-rays). Eleni Adamidi and her collaborators identified 38 such studies, most of which demonstrated high accuracy [107]. One team of Chinese researchers, responding to the crisis in Wuhan, was able to create a tool for both diagnosis and prognosis in two months. This was then made available for use in “an epidemic area and two non-epidemic areas in China”, as well as globally, in the “hope that this can assist [the] management of patients, and [that] the data … input may further perfect our AI system, which we hope can evolve as a versatile tool for the global community to combat COVID and other emerging viral infections” [116, 81; see also the discussion of “AI-assisted diagnosis in 110].
The pandemic also boosted use of more general-purpose diagnostic tools. iFlyTek, one of China’s largest AI and speech-technology companies, developed an AI Medical Assistant that is in use nationwide. The company recently reported that it “has been adopted in over 30,000 local medical institutions and [is] serving more than 50,000 grassroots doctors; assisting in more than 200 million diagnoses.” Healthcare staff enter a patient’s symptoms into the Medical Assistant, and it provides advice on a possible diagnosis [81, 127]. Its usage, although still modest, is growing rapidly and already exceeds “pilot” or “experimental” scale. This reality contrasts with an assessment of the state of medical AI adoption in a just published case study, according to which “the use of AI in healthcare is still in its early stages, …[and] because the medical field involves human life and health problems, it presents unique characteristics. Until the technology is fully mature, its promotion and application will be relatively slow” [128].
Among the reasons why adoption has, in fact, quickened, is that diagnostic tools that can be used remotely meet several key policy goals for healthcare:
- Enable contactless screening and sometimes treatment, reducing the risk of infection.
- Help “rebalance the distribution of medical services, linking better medical resources in East China with demands in the central and western areas”; redress the imbalance of medical care between urban and rural areas.
- Achieve greater efficiencies at lower cost [129].
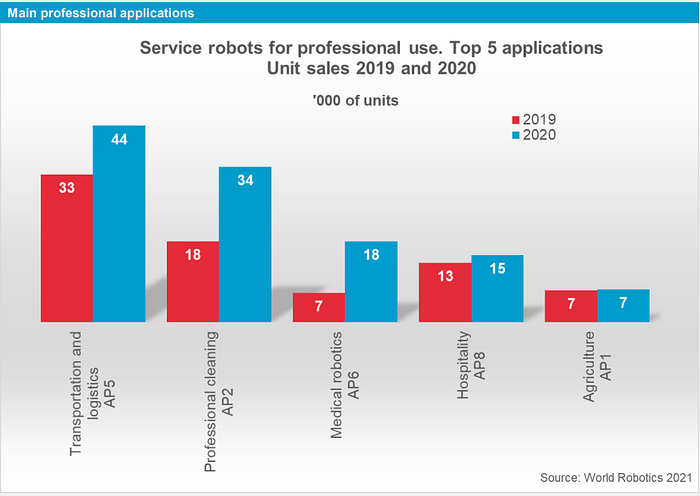
Robotics. The pandemic prompted a dramatic surge in global demand for service robots in 2020, with unit sales up 33% for transportation applications, 88% for professional cleaning, and an astonishing 157% for medical robotics.
Robots can play a variety of useful roles in pandemic response, including
- Sanitation and disinfection in hospitals and public spaces.
- Delivery inside hospitals.
- Delivery outside hospitals, including both “last-mile” and longer intra-urban routes.
- Patrolling.
- Screening and monitoring.
- Collecting throat swabs [108, 118].
All of these rely in part on artificial intelligence, particularly because robots in these roles act with varying degrees of autonomy.
Many robotic applications are dual-purpose. Disinfection robots not only prevent viral transmission but increase capacity in short-staffed hospitals and other facilities. Similarly, autonomous delivery robots not only provide a contactless service but compensate for labor shortages.
Chinese institutions have been among the most adroit at taking advantage of the potential of robotics to assist in pandemic management. A prime example of this was CloudMinds’ setup of a wholly robotic ward in a Wuhan field hospital. CloudMinds provides a cloud-based robot operating system. As their CEO, Bill Huang, explained in a June 2020 interview, “On 24 January, the day after the Chinese government imposed a lockdown on the city of Wuhan, we shifted our company’s focus to help to fight the spread of the virus. Since the outbreak, all Chinese robot companies that I know of have done this.” A month later, the company began setting-up “China’s first robot-run ward.” By March 6, “we had 12 robots performing different functions, ranging from the delivery of food, drinks and drugs, to monitoring vital signs and disinfecting the area. Outside the room, clinical staff controlled and monitored the robots’ movements” [119, 120]. Although this proved to be a short-lived trial — the temporary hospital itself was soon no longer needed — it illustrates the agility and sense of shared purpose that has informed the use of technology in China’s response to COVID. Moreover, the robotic functions deployed in this trial are becoming widely used in Chinese hospitals, quarantine centers, and beyond.
- Over 30,000 robots were already deployed in kindergartens throughout China, primarily for health screening. Screening for COVID was added [122].

- Many hospitals in China have adopted disinfection robots. As SaniPass, a company specializing in institutional disinfection solutions, noted, “China was a trend-setter in this field, using disinfection robots in healthcare early in the course of the pandemic” [123]. Some, such as XDBot, developed by Nanyang Technological University, “can outcompete human cleaning capacity” [108]. Robots are also being used in hospitals to perform “diagnoses, take samples and carry out thermal imaging” [124].
- Use of self-driving vehicles for “delivery of medication, food, documents, and infectious samples for testing” is growing. Some can travel up to 100 km with up to 100 kg of goods, making multiple deliveries. Others are designed for use in nonmotorized areas for “last-mile” delivery [108]. The pandemic as hastened rollout plans, and adoption appears to be at an inflection point due to falling production costs, increasing competency and reliability, and the benefits of early experience [126].
- Robots are being used in quarantine hotels “to monitor the quarantine situation and deliver food, bottled water, and other packages to those self-isolating” [108]. Some also take guests’ temperatures [125].
- Disinfection and delivery robots will be widely used during the Beijing Winter Games [121].
5 Conclusions
China stands nearly alone in having successfully implemented and sustained, for nearly two years, a zero-COVID policy. Although this is being tested by the omicron variant, it is very likely to be sustained, in part because the capability exists to do so, but largely because it is hard to imagine decision makers in China deciding that the alternative — conditions in the EU, the United States, and elsewhere — are preferable [141].
It is, rather, societies and leaders outside China that could benefit from China’s example. This is not only because China has suffered far less illness and loss of life, and done much better economically, during the pandemic. In addition, and critically, had the world possessed the capacity and political will to employ a zero-COVID strategy like China’s, there would probably be no omicron variant today, and COVID would not continue to ravage human societies. The inability or unwillingness of most other nations to adopt a zero-COVID policy has had far-reaching consequences, but these have been limited by COVID’s relatively low case fatality rate (CFR) as well as by the development of vaccines and, soon, anti-viral drugs. A future pandemic could be worse [130].
In the sections above I’ve tried to characterize the chief factors — governmental, technical, and social — that account for the continued success of China’s pandemic strategy. These factors, summarized below, are interdependent; suppressing COVID requires integrated use of them.
National commitment, mobilization, and coordination. Government must provide visionary leadership. In China’s case, the early articulation of a “people first” commitment was essential. First, it oriented the entire subsequent effort. Second, it clearly conveyed to the governmental, party, and corporate leadership that a temporary failure to achieve economic goals was acceptable (this was also spelled-out in other ways). Third, it constituted a promise to the Chinese people and staked the government’s — and more the party’s — continued legitimacy on the success of a zero-COVID policy. This reassured and engaged citizens, and was a pervasive reminder that the impositions of the policy served a critical collective purpose. The extraordinary mobilization that began with the rescue of Wuhan was based on the policy commitment but was also, of course, both a test of and a demonstration of it. It proved that the government’s — and the healthcare system’s, as well as ordinary citizens’ — commitment was both real and effective, and could be counted on. Lastly, varied resources from every sector and throughout the country were coordinated to achieve and sustain success. Coordination has not been perfect, but it has been encompassing, and it has improved over time.
An important element of the zero-COVID policy, and a major factor in its acceptance, were the many measures taken to reorient and expand social welfare programs to aid people and small- and medium-sized businesses.
Existing social insurance programs, the MLSS, and some special temporary policy arrangements have been combined to circumvent the sharp increase in social suffering. [These include] (1) cash payments such as unemployment allowances and unemployment subsidies, benefits from the Chinese social assistance program (MLSS), ensuring the material security of millions of people and employees who have suffered from temporary layoffs, shortened workhours, or mandatory breaks imposed by employers; (2) benefits in kind, including service programs like testing, diagnosis, and therapy for Covid-19 patients, free of charge, either financed by health insurance programs or subsidized by state revenues. Also included are special social protection and social services for elderly people in nursing homes and social welfare units who constitute one of thehighly vulnerable groups exposed to the virus; (3) favorable policy measures, such as the alleviation of income tax burdens and the granting of special loans for small- and medium-sized enterprises who face challenges in existential survival owing to a lack of liquidity because of the drastic freeze in economic and commercial activities [131].
Lastly, and important to note, is that the Chinese public has “paid unprecedented attention to self-protection”, including masking, social distancing, use of sanitizers, and limitations on social gatherings where warranted. “Hence, even for regions where the government did not strictly impose face masks, people would wear a face-mask and use sanitisers in public” [135].
Social solidarity and institutional trust. The essential role of solidarity was recognized very early in the pandemic response. As Bruce Aylward, Senior Advisor to the WHO’s Director-General, noted at the press conference reporting on the results of the Joint Mission on February 24, pandemic control “can’t work without the collective will of the population contributing to it” [50]. It is, in this respect, instructive that Taiwan, rated one of the world’s most democratic countries, provides another example of a successful zero COVID strategy [23, 24, 25]. Solidarity has specific practical implications, as Yasheng Huang and his collaborators noted:
What, then, do the countries that have so far been effectively flattening the curve have in common? Part of the answer is that they tend to be in East Asia — China, South Korea, Taiwan, Singapore and to a lesser extent Japan — where a collectivist spirit may encourage civic-minded embrace of and a more willing compliance with governments’ infection control. In addition, these countries tend to be actively deploying technology to collect data on the virus’s progress and efforts to contain it, including tracking those who are infected and their contacts. These two aspects of East Asian societies do not work independently; they reinforce each other [59].
Targeted and mass testing. Testing is used promptly and at varying scales to accurately delineate the scope of outbreaks in order to precisely shape the response, resulting in faster, more effective containment while minimizing adverse impacts on people and businesses.
Beginning in Wuhan, the government has, on a number of occasions, conducted rapid testing of all residents in areas with outbreaks. As Zhongjie Li and his co-authors put it, these “risk-based, large-scale, population-wide screenings contributed to case finding and rapid control of epidemics and provided evidence for the government to reopen economic activities” [39]. There are a number of notable features of these events:
- The purpose is clear: to establish a trustworthy, complete identification of positive cases and close contacts. This can be critical to containing an outbreak or to ensuring that it has been contained, enabling social and economic activities to fully resume while providing detailed information on where targeted quarantines and other pandemic management efforts should be focused.
- Testing of millions — 10 million, in the case of Wuhan — within very short periods is an impressive technical and administrative accomplishment.
- The attainment of near universal participation attests to public support for the zero-COVID policy, buttressed by the fact that a negative test contributes to a green Health Code rating, ensuring freedom of movement.
Mass testing is, however, a last resort, in cases where targeted testing and control measures have failed or are insufficient. More commonly, new outbreaks are identified and suppressed quickly. Overall, China has actually conducted far fewer tests than the United States, because it has not needed to [142].
Digital contact tracing. The high transmissibility of COVID, worsened by the delta and now omicron variants, means that traditional manual contact tracing is quickly overwhelmed during outbreaks. In addition, high transmissibility worsens the consequences people’s forgetfulness and gaps in their situational knowledge as well as the difficulties of reaching them and persuading them to participate. For all these reasons, the near universal adoption of digital contact tracing has been a lynchpin of China’s success. Tracing is much quicker and more thorough, making possible the targeted management of outbreaks that ensures responses are economical, efficient, and impose restrictions only where necessary and not society wide.
Use of Health Code apps. Swift adoption and pervasive use of the Health Code apps has been instrumental in providing a flexible, individualized framework for regulating movement to minimize the risk of transmission. They connect people dynamically with provincial and national pandemic information management systems while providing an effective way to gatekeep access to public spaces based on risk. They enable testing, contact tracing, and other health data to be integrated and to inform the key risk decisions embodied in the red-yellow-green codes.
Closed community management. Widespread use of “circle-layer” and other types of closed community management has enabled China to conduct highly circumscribed quarantines and to significantly reduce the risk of transmission. As Zhu Qingyi explains, “Urban communities and village communities are administratively defined units for social governance in China. Communities provide geographical space for residents’ daily activities. China adopted closed-off community management right after COVID-19 broke out. Common measures include but are not limited to minimizing entrance numbers, setting up checking points, issuing entry permits, supervising face mask wearing, enhancing health monitoring and registering personnel and vehicles passing through.” Closed-off management “effectively decreases people flows, protects vulnerable populations and curbs virus spread” [133].
Restrictions on inter-provincial and inter-urban movement. China first imposed restrictions on movement across provinces at the outset of the crisis in Wuhan, in part because it coincided with the start of the Spring Festival, ordinarily the time of greatest movement within the country. As the figure below shows, outflow from Wuhan was almost completely halted for a time [134].
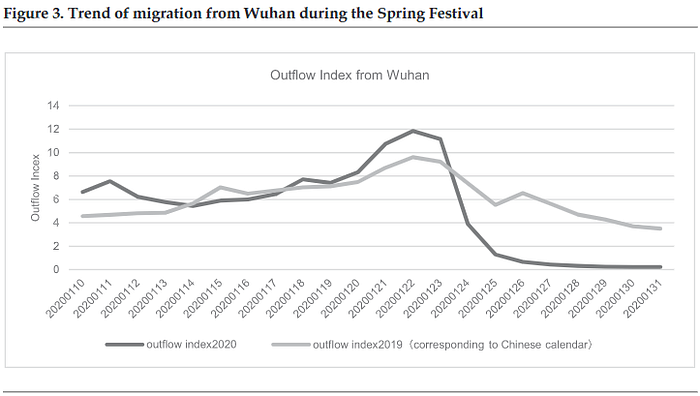
Subsequent research has established “that secondary epicenters such as Beijing, Guangdong, and Shanghai, developed at a very early stage of the outbreak …[and] mobility restrictions across regions indeed prevented the further spread of the disease.” Indeed, if “the primary goal is to eliminate the disease entirely, the central and local governments must implement preventive measures simultaneously”. It seems important to note that, according to Tatsushi Oka and his collaborators, the decrease in cross-region mobility has been “largely due to travelers acting precautionarily and voluntarily canceling their travel plans” [135].
The role of artificial intelligence. Until now, AI’s diverse contributions to pandemic management in China appear to have assisted or enhanced efforts that would have succeeded without it. However, its importance is growing rapidly. It already plays a significant role in diagnostics and in robotics applications, and it is on the threshold of wider usage in many other areas, including triage, prognosis, epidemiological pattern recognition and prediction, virology and pathogenesis, and drug and vaccine development.
The use of AI in the containment of COVID in China is a virtuous circle. Its ability to contribute to improvements in diagnosis, robotics, drug discovery, and in other areas depends on the availability of large datasets for training and discovery. In turn, AI utilization is a learning experience that feeds improvement processes. More broadly, as Kai-Fu Lee explains, harnessing the power of AI requires four inputs: “abundant data, hungry entrepreneurs, AI scientists, and an AI-friendly policy environment” [99]. In its response to COVID, China is demonstrating that it has all of these in abundance.
5.1 Can We Learn?
The remarkably effective response of China’s State Council and Chinese society to the pandemic has been overshadowed in the US and throughout much of the world by criticism of China for mismanaging the initial outbreak and for its authoritarianism. Particularly in the case of the Trump administration, the rhetoric of blame served to distract attention from its own pandemic response failures. There is evidence for the prevalence of the same kind of rhetoric in the media of many countries.
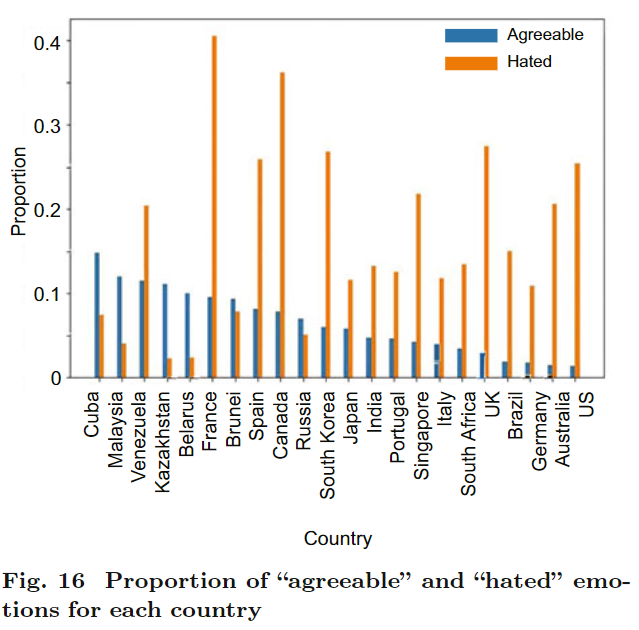
A major study that used supervised deep learning to analyze more than 280,000 news items from 57 mainstream sources in 22 countries from December 1, 2019 to June 30, 2020 found that negative items substantially outweighed positive ones, particularly in the areas of “society”, “economy”, and “politics”. And when examining emotional tone, where emotions were categorized as “agreeable, believable, good, hated, worried, and sad”, the emotion labelled “hated” predominated in 15 of the 22 countries, often by a wide margin (see Figure 16 from the study below). In the U.S, 62% of items were in the “hated” category and only 3% were “agreeable” (the second largest category was “worried” at 32%) [153].
Other, more narrowly focused research reached similar conclusions. A study of coverage of the earliest phase of the pandemic — January through April 2020 — by three influential papers, The New York Times, The Times (of London), and The Guardian, found that it was “dominated by negative attitudes, with 30–50 percent neutral coverage, and with relatively little positive coverage.” Even after China gained control of the epidemic, coverage remained negative, with the predominant narrative for the period that of an “epidemic paralyzed China who adopts ineffective epidemic prevention measures.” What did change is that there was simply less reporting [154]. And a frame analysis of eight U.S. news sources across the political spectrum from January through June found that three-quarters of the items were negatively framed [155].
While it is difficult to prove a causal relationship between media coverage and public attitudes and beliefs, what is certain is that “unfavorable opinion [of China] has soared”, according to a global opinion survey by Pew Research. “Across the 14 nations surveyed, a median of 61% say China has done a bad job dealing with the outbreak” [156].
We are unlikely to learn as long as China is blamed for the pandemic in media coverage and public opinion, and as long as the elements of its successful pandemic management are under-reported and, when covered, typically framed as examples of heavy-handed authoritarianism.
What is especially troubling about this is not only that we tolerate an enormous loss of life and substantial economic harm that we possess the technical and administrative means to avoid, but that our choice to do so is only at all viable because this pandemic is relatively mild. Were COVID’s case fatality rate much worse, the pandemic management policy of the US and most of the world outside East Asia would have horrific consequences. By refusing — so far — to learn from and adapt China’s approach to democracies, we render ourselves unprepared for a worse “next time”, despite the fact that a next time of some sort is likely. And we sustain the very conditions which enable SARS-CoV-2 to continue evolving and which will do the same for any future pandemic. Lastly, blaming China not only distracts from but undermines the urgent need to invest in and build a far better global system for disease monitoring and management.
References
- Our World in Data. (2021). “China: Coronavirus Pandemic Country Profile.” Our World in Data. https://ourworldindata.org/coronavirus/country/china.
- Our World in Data. (2021). “United States: Coronavirus Pandemic Country Profile.” Our World in Data. https://ourworldindata.org/coronavirus/country/united-states.
- Liu, Jiangmei, Lan Zhang, Yaqiong Yan, Yuchang Zhou, Peng Yin, Jinlei Qi, Lijun Wang, et al. 2021. “Excess Mortality in Wuhan City and Other Parts of China during the Three Months of the Covid-19 Outbreak: Findings from Nationwide Mortality Registries.” BMJ (Online) 372: n415. https://doi.org/10.1136/bmj.n415.
- Li, Zhongjie, Xuhua Guan, Naiying Mao, Huiming Luo, Ying Qin, Na He, Zhen Zhu, et al. 2021. “Antibody Seroprevalence in the Epicenter Wuhan, Hubei, and Six Selected Provinces after Containment of the First Epidemic Wave of COVID-19 in China.” The Lancet Regional Health — Western Pacific 8 (March): 94. https://doi.org/10.1016/J.LANWPC.2021.100094.
- Gan, Nectar. 2020. “True Toll of Wuhan Infections May Be Nearly 10 Times Official Number, Chinese Researchers Say.” CTV News. December 29, 2020. https://www.ctvnews.ca/health/coronavirus/true-toll-of-wuhan-infections-may-be-nearly-10-times-official-number-chinese-researchers-say-1.5247063.
- Cukierman, Alex. 2020. “Why Is COVID-19 Incidence in Authoritarian China so Much Lower than in the Democratic US: Effectiveness of Collective Action or Chinese Cover-up?” VoxEu. October 26, 2020. https://voxeu.org/content/why-covid-19-incidence-authoritarian-china-so-much-lower-democratic-us-effectiveness-collective-action-or-chinese-cover. “During the initial phases of Wuhan’s major outbreak of the virus, the Chinese Communist Party (CCP) actively suppressed information about the emerging pandemic, delayed the publication of information about the fact that it is transmitted from human to human, and swiftly suspended millions of informative messages on WeChat and similar outlets that were relaying information from medical stuff about the dire medical situation in Wuhan to colleagues in the rest of China. Dr Li Wenliang at Wuhan City Central Hospital had been silenced by the police after warning about the new coronavirus that has killed hundreds in China and sickened thousands. Shortly after, he died from the virus. His death ignited responses from people with different backgrounds, including government officials, prominent business figures and ordinary online users. They have posted numerous messages expressing their grief for the doctor and their anger over his silencing by the police. Most of the accounts of the message senders were closed after a while by the CCP.”
- Hernández, Javier C. 2020. “In China, Where the Coronavirus Pandemic Began, Life Is Starting to Look Normal.” The New York Times. August 23, 2020. https://www.nytimes.com/2020/08/23/world/asia/china-coronavirus-normal-life.html.
- Hernández, Javier C. 2020. “How China Brought Nearly 200 Million Students Back to School .” The New York Times. September 12, 2020. https://www.nytimes.com/2020/09/12/world/asia/china-schools-reopening.html.
- Ho, Ryan. 2021. “Commentary: China’s COVID-19 Successes — Credible at Home, Not so Much Abroad.” CNA. July 2, 2021. https://www.channelnewsasia.com/commentary/china-covid-19-coronavirus-success-how-credible-cases-stats-real-1995066.
- World Bank. 2021. “China Overview: Development News, Research, Data.” World Bank. October 12, 2021. https://www.worldbank.org/en/country/china/overview#1.
- BBC News. 2021. “China’s Economy Grows 18.3% in Post-Covid Comeback.” BBC News. April 16, 2021. https://www.bbc.com/news/business-56768663.
- SARS-CoV-2 stands for “severe acute respiratory syndrome coronavirus 2.” It is the virus that causes the disease COVID-19 in humans. In animals, SARS-CoV-2 also refers to the disease.
- Wikipedia contributors. 2021. “COVID-19 pandemic in Hubei.” Wikipedia, The Free Encyclopedia. October 5, 2021. https://en.wikipedia.org/w/index.php?title=COVID-19_pandemic_in_Hubei&oldid=1048253859.
- World Health Organization. 2021. “WHO-Convened Global Study of Origins of SARS-CoV-2: China Part.” https://www.who.int/publications/i/item/who-convened-global-study-of-origins-of-sars-cov-2-china-part.
- Wikipedia contributors. 2021. “Investigations into the Origin of COVID-19.” Wikipedia, The Free Encyclopedia. October 26, 2021. https://en.wikipedia.org/wiki/Investigations_into_the_origin_of_COVID-19.
- Tufekci, Zeynep. 2021. “Where Did the Coronavirus Come From? What We Already Know Is Troubling.” The New York Times. June 25, 2021. https://www.nytimes.com/2021/06/25/opinion/coronavirus-lab.html.
- Zhang, Hong. 2020. “Early Lessons from the Frontline of the 2019-NCoV Outbreak.” The Lancet (British Edition) 395 (10225): 687. https://doi.org/10.1016/S0140-6736(20)30356-1.
- Sun, Shuangyi, Zhen Xie, Keting Yu, Bingqian Jiang, Siwei Zheng, and Xiaoting Pan. 2021. “COVID-19 and Healthcare System in China: Challenges and Progression for a Sustainable Future.” Globalization and Health 17 (1): NA-NA. https://doi.org/10.1186/S12992-021-00665-9.
- Ang, Yuen Yuen. 2020. “When COVID-19 Meets Centralized, Personalized Power.” Nature Human Behaviour 2020 4:5 4 (5): 445–47. https://doi.org/10.1038/s41562-020-0872-3.
- Office of the Director of National Intelligence. National Intelligence Council. 2021. “Updated Assessment on COVID-19 Origins.” https://www.dni.gov/files/ODNI/documents/assessments/Declassified-Assessment-on-COVID-19-Origins.pdf.
- Ning, Yan, Ran Ren, and Gerard Nkengurutse. 2020. “China’s Model to Combat the COVID-19 Epidemic: A Public Health Emergency Governance Approach.” Global Health Research and Policy 5 (1). https://doi.org/10.1186/S41256-020-00161-4.
- Liu, Yu, and Richard B. Saltman. 2020. “Policy Lessons From Early Reactions to the COVID-19 Virus in China.” American Journal of Public Health 110 (8): 1145. https://doi.org/10.2105/AJPH.2020.305732.
- Wikipedia contributors. (2021, November 2). Democracy Index. In Wikipedia, The Free Encyclopedia. Retrieved 00:18, November 4, 2021, from https://en.wikipedia.org/w/index.php?title=Democracy_Index&oldid=1053198042.
- Taiwan COVID: 16,428 Cases and 847 Deaths — Worldometer (worldometers.info).
- Brugha, Ruairi. 2021. “Zero COVID Worked for Some Countries — but High Vaccine Coverage Is Now Key.” The Conversation. October 12, 2021. https://theconversation.com/zero-covid-worked-for-some-countries-but-high-vaccine-coverage-is-now-key-169327.
- Lu, Donna. 2020. “How China Is Beating Covid-19.” New Scientist (1971) 248 (3311): 10–11. https://doi.org/10.1016/S0262-4079(20)32107-2.
- Jinping, Xi. 2020. “Xi Jinping Gives Important Instructions on the Outbreak of Pneumonia, a New Type of Coronavirus Infection.” Xinhua News Agency. January 20, 2020. http://www.gov.cn/xinwen/2020-01/20/content_5471057.htm.
- Qian, Xu, Ran Ren, Youfa Wang, Yan Guo, Jing Fang, Zhong Dao Wu, Pei Long Liu, and Tie Ru Han. 2020. “Fighting against the Common Enemy of COVID-19: A Practice of Building a Community with a Shared Future for Mankind.” Infectious Diseases of Poverty 9 (1). https://doi.org/10.1186/S40249-020-00650-1.
- Tian, Huaiyu, Yonghong Liu, Yidan Li, Chieh Hsi Wu, Bin Chen, Moritz U.G. Kraemer, Bingying Li, et al. 2020. “An Investigation of Transmission Control Measures during the First 50 Days of the COVID-19 Epidemic in China.” Science 368 (6491): 638–42. https://doi.org/10.1126/SCIENCE.ABB6105.
- AlTakarli, Nourah S. 2020. “China’s Response to the COVID-19 Outbreak: A Model for Epidemic Preparedness and Management.” Dubai Medical Journal 3 (2): 44–49. https://doi.org/10.1159/000508448.
- Conant, Eve. 2020. “What Would a 60 Million Person Lockdown Look Like?” National Geographic. March 13, 2020. https://www.nationalgeographic.com/history/article/60-million-person-coronavirus-lockdown-united-states.
- Wikipedia contributors. (2021, October 28). COVID-19 lockdown in China. In Wikipedia, The Free Encyclopedia. Retrieved 06:00, November 4, 2021, from https://en.wikipedia.org/w/index.php?title=COVID-19_lockdown_in_China&oldid=1052367685.
- Johns Hopkins Coronavirus Resource Center. 2020. “Hubei Timeline.” Johns Hopkins Coronavirus Resource Center. 2020. https://coronavirus.jhu.edu/data/hubei-timeline.
- Xiaodong, Wang, and Wu Yong. 2020. “Entire Nation Mobilizes to Help Wuhan.” China Daily. February 27, 2020. https://www.chinadaily.com.cn/a/202002/27/WS5e571e90a31012821727aae0.html.
- Wikipedia contributors. (2021, May 14). Fangcang hospital. In Wikipedia, The Free Encyclopedia. Retrieved 21:08, November 4, 2021, from https://en.wikipedia.org/w/index.php?title=Fangcang_hospital&oldid=1023073663.
- Chen, Simiao, Zongjiu Zhang, Juntao Yang, Jian Wang, Xiaohui Zhai, Till Bärnighausen, and Chen Wang. 2020. “Fangcang Shelter Hospitals: A Novel Concept for Responding to Public Health Emergencies.” The Lancet 395 (10232): 1305–14. https://doi.org/10.1016/S0140-6736(20)30744-3.
- The Straits Times. 2020. “Coronavirus: Wuhan to Build 19 More Makeshift Hospitals as China Struggles to Contain Epidemic, East Asia News & Top Stories.” The Straits Times. February 21, 2020. https://www.straitstimes.com/asia/east-asia/coronavirus-wuhan-to-activate-one-more-temporary-hospital-with-3690-beds.
- Villains, Oscar, Lynn Beyak, and Anne Quito. 2020. “How China Built Two Hospitals in Two Weeks to Combat the Coronavirus.” CBC Radio. February 7, 2020. https://www.cbc.ca/radio/day6/oscar-villains-lynn-beyak-coronavirus-hospitals-weinstein-s-lawyer-the-creator-of-comic-sans-and-more-1.5454398/how-china-built-two-hospitals-in-two-weeks-to-combat-the-coronavirus-1.5454409.
- Li, Zhongjie, Fengfeng Liu, Jinzhao Cui, Zhibin Peng, Zhaorui Chang, Shengjie Lai, Qiulan Chen, Liping Wang, George F. Gao, and Zijian Feng. 2021. “Comprehensive Large-Scale Nucleic Acid–Testing Strategies Support China’s Sustained Containment of COVID-19.” Nature Medicine 2021 27:5 27 (5): 740–42. https://doi.org/10.1038/S41591-021-01308-7.
- Chen, Yawen, and Cate Cadell. 2020. “Confusion and Lost Time: How Testing Woes Slowed China’s Coronavirus Response.” Reuters. January 27, 2020. https://www.reuters.com/article/us-china-health-testing-insight/confusion-and-lost-time-how-testing-woes-slowed-chinas-coronavirus-response-idUSKBN1ZQ21K.
- Hong, Zhao. 2020. “What Role Did China’s Testing Play in Containing the Spread of COVID-19?” CGTN. April 23, 2020. https://news.cgtn.com/news/2020-04-23/Graphics-How-has-China-s-testing-helped-contain-spread-of-COVID-19--PVH0n9o760/index.html.
- The State Council Information Office of the People’s Republic of China. 2020. “Fighting COVID-19: China in Action.” Wikisource, the Free Online Library. June 2020. https://en.wikisource.org/wiki/Fighting_COVID-19:_China_in_Action. Also of note, the State Council reported that its Joint Prevention and Control Mechanism had “strengthened coordination, which made it possible for the supply of medical N95 masks to exceed Hubei’s requirement” on February 5. Similarly, the State Council reports that “the supply of medical protective suits to Hubei exceeded its needs” on February 11.
- According to the State Council [42], the National Health Commission (NHC) “released Diagnosis and Treatment Protocol for Novel Coronavirus Pneumonia (Trial Version 5)” on February 5. If this is correct, it only impacted reporting in Hubei a week later.
- This assistance is probably what is being referred to in the State Council report [42] when it states “February 10: A mechanism was established to organize pairing assistance from other provinces to Hubei’s cities other than Wuhan for treatment of the infected. Assistance from 19 provinces was rendered to 16 cities in Hubei.”
- Statistics Times. 2021. “Countries by GDP Growth 2020.” StatisticsTimes.Com. October 24, 2021. https://statisticstimes.com/economy/countries-by-projected-gdp-growth.php.
- Cao, Shiyi, Yong Gan, Chao Wang, Max Bachmann, Shanbo Wei, Jie Gong, Yuchai Huang, et al. 2020. “Post-Lockdown SARS-CoV-2 Nucleic Acid Screening in Nearly Ten Million Residents of Wuhan, China.” Nature Communications 2020 11:1 11 (1): 1–7. https://doi.org/10.1038/s41467-020-19802-w.
- Huang, Chaolin, Yeming Wang, Xingwang Li, Lili Ren, Jianping Zhao, Yi Hu, Li Zhang, et al. 2020. “Clinical Features of Patients Infected with 2019 Novel Coronavirus in Wuhan, China.” The Lancet 395 (10223): 497–506. https://doi.org/10.1016/S0140-6736(20)30183-5/ATTACHMENT/D5332CA1-83D8-4C4C-BC57-00A390BF0396/MMC1.PDF.
- Pekar, Jonathan, Michael Worobey, Niema Moshiri, Konrad Scheffler, and Joel O. Wertheim. 2021. “Timing the SARS-CoV-2 Index Case in Hubei Province.” Science 372 (6540): 412–17. https://doi.org/10.1126/SCIENCE.ABF8003.
- For an overview of the organization of the national response, see “Centralized and Efficient Command” in “Fighting COVID-19: China in Action” [42]. “Emergency command mechanisms headed by leading Party and government officials were established in provinces, cities and counties across the country, forming a top-down system with unified command, frontline guidance, and coordination between departments and among provinces”.
- World Health Organization. 2020. “Press Conference of WHO-China Joint Mission on COVID-19.” World Health Organization. February 24, 2020. https://www.who.int/docs/default-source/coronaviruse/transcripts/joint-mission-press-conference-script-english-final.pdf.
- Page, Jeremy. 2020. “Wuhan Tests Show Coronavirus ‘Herd Immunity’ Is a Long Way Off.” The Wall Street Journal, April 16, 2020. The State Council report was more emphatic on the existence of two rounds of testing: “Wuhan carried out two rounds of community-based mass screening of its 4.21 million households, leaving no person or household unchecked and ruling out all potential sources of infection” [42].
- Wee, Sui-Lee, and Vivian Wang. 2020. “Here’s How Wuhan Tested 6.5 Million for Coronavirus in Days.” The New York Times. June 3, 2020. https://www.nytimes.com/2020/05/26/world/asia/coronavirus-wuhan-tests.html.
- Reuters Staff. 2020. “No New COVID Sufferers, 300 Asymptomatic, after Wuhan-Wide Tests.” Reuters. June 2, 2020. https://www.reuters.com/article/us-health-coronavirus-china-wuhan/no-new-covid-sufferers-300-asymptomatic-after-wuhan-wide-tests-idUSKBN23915R.
- Atripaldi, Luigi, Silvia Sale, Mariaelena Capone, Vincenzo Montesarchio, Roberto Parrella, Gerardo Botti, Paolo Antonio Ascierto, and Gabriele Madonna. 2021. “Could Asymptomatic Carriers Spread the SARS-CoV-2 Infection? Experience from the Italian Second Wave.” Journal of Translational Medicine 19 (1): 1–4. https://doi.org/10.1186/S12967-021-02762-0/TABLES/2.
- Johansson, Michael A., Talia M. Quandelacy, Sarah Kada, Pragati Venkata Prasad, Molly Steele, John T. Brooks, Rachel B. Slayton, Matthew Biggerstaff, and Jay C. Butler. 2021. “SARS-CoV-2 Transmission From People Without COVID-19 Symptoms.” JAMA Network Open 4 (1): e2035057–e2035057. https://doi.org/10.1001/JAMANETWORKOPEN.2020.35057.
- Nye, Jessica. 2021. “CDC: Most Transmission of COVID-19 Likely From Asymptomatic or Presymptomatic Individuals.” Infectious Disease Advisor. February 12, 2021. https://www.infectiousdiseaseadvisor.com/home/topics/covid19/cdc-determines-at-least-half-of-coronavirus-infections-transmitted-by-asymptomatic-individuals/.
- Fu, Han, Haowei Wang, Xiaoyue Xi, Adhiratha Boonyasiri, Yuanrong Wang, Wes Hinsley, Keith J Fraser, et al. 2021. “Database of Epidemic Trends and Control Measures during the First Wave of COVID-19 in Mainland China.” International Journal of Infectious Diseases 102: 463–71. https://doi.org/10.1016/j.ijid.2020.10.075.
- Wang, Huan, Markus Zhang, Robin Li, Oliver Zhong, Hannah Johnstone, Huan Zhou, Hao Xue, et al. 2021. “Tracking the Effects of COVID-19 in Rural China over Time.” International Journal for Equity in Health 20 (1): NA-NA. https://doi.org/10.1186/S12939-020-01369-Z.
- Huang, Yasheng, Meicen Sun, and Yuze Sui. 2020. “How Digital Contact Tracing Slowed Covid-19 in East Asia.” Harvard Business Review. April 15, 2020. https://hbr.org/2020/04/how-digital-contact-tracing-slowed-covid-19-in-east-asia.
- Huang, Yasheng. 2020. “No, Autocracies Aren’t Better for Public Health | Boston Review.” Boston Review. April 14, 2020. https://bostonreview.net/politics-global-justice/yasheng-huang-no-autocracies-arent-better-public-health.
- Wikipedia contributors. (2021, November 14). COVID-19. In Wikipedia, The Free Encyclopedia. Retrieved 18:48, November 15, 2021, from https://en.wikipedia.org/w/index.php?title=COVID-19&oldid=1055235862.
- Wang, J., & Du, G. (2020). COVID-19 may transmit through aerosol. Irish journal of medical science, 189(4), 1143–1144. https://doi.org/10.1007/s11845-020-02218-2.
- Centers for Disease Control and Prevention. (2021, August 26). Delta Variant: What We Know About the Science. Centers for Disease Control and Prevention. https://www.cdc.gov/coronavirus/2019-ncov/variants/delta-variant.html.
- Boeing, Philipp, and Yihan Wang. 2021. “Decoding China’s COVID-19 ‘Virus Exceptionalism’: Community-Based Digital Contact Tracing in Wuhan.” R&D Management 51 (4): 339–51. https://doi.org/10.1111/RADM.12464.
- Shahroz, Muhammad, Farooq Ahmad, Muhammad Shahzad Younis, Nadeem Ahmad, Maged N. Kamel Boulos, Ricardo Vinuesa, and Junaid Qadir. 2021. “COVID-19 Digital Contact Tracing Applications and Techniques: A Review Post Initial Deployments.” Transportation Engineering 5 (September): 100072. https://doi.org/10.1016/J.TRENG.2021.100072.
- Liang, Fan. 2020. “COVID-19 and Health Code: How Digital Platforms Tackle the Pandemic in China.” Social Media + Society 6 (3): 2056305120947657. https://doi.org/10.1177/2056305120947657.
- Chen, Mengji, Shan Xu, Lewis Husain, and Gauden Galea. 2021. “Digital Health Interventions for COVID-19 in China: A Retrospective Analysis.” Intelligent Medicine 1 (1): 29–36. https://doi.org/10.1016/J.IMED.2021.03.001.
- Yang, F., Heemsbergen, L., and Fordyce, R. (2020). “Comparative analysis of China’s Health Code, Australia’s COVIDSafe and New Zealand’s COVID Tracer Surveillance Apps: a new corona of public health governmentality?” Media International Australia, 178 (1), 182–197. https://doi.org/10.1177/1329878X20968277.
- Wang, J. (2021, May 6). “China: The QR Code System — a battle between privacy and public interests?” Lex-Atlas. https://lexatlas-c19.org/the-use-of-qr-code-system-in-china-a-battle-between-protecting-privacy-and-safeguarding-public-interests/.
- A series of national standards on personal health information code were issued on April 29, 2020 by the State Administration for Market Regulation (SAMR) and the Standardization Administration of China (SAC) via a rapid channel, which only took 14 days from project approval to publication. The standards, developed by SAC/TC 28 on information technology, include GB/T 38961–2020, Personal health information code — Reference model, GB/T 38962–2020, Personal health information code — Data format, and GB/T 38963–2020, Personal health information code — Application interface. After implementation, they can help guide the design, development and system integration of relevant information system for health code.
- Stancheva, T. (2021, July 4). “21 Mind-Blowing WeChat Statistics You Should Know in 2021.” Review 42. https://review42.com/resources/wechat-statistics/.
- Statista. (2021). “Number of monthly active users of leading payment apps 2021.” Statista. https://www.statista.com/statistics/1211923/china-leading-payment-apps-based-on-monthly-active-users/.
- Kim, Hyunju, and Ayan Paul. 2021. “Automated Contact Tracing: A Game of Big Numbers in the Time of COVID-19.” Journal of the Royal Society Interface 18 (175). https://doi.org/10.1098/rsif.2020.0954.
- Dong, Mengyu. 2021. “‘Mini-Programs’ Took over Chinese Platforms. Now They’re Being Used to Contact Trace — and Undermine Privacy.” Rest of World. September 28, 2021. https://restofworld.org/2021/mini-programs-china/.
- Office of the Central Committee for Cybersecurity and Information Technology. (2020, February 4). “notice on the protection of personal information and the use of big data to support joint prevention and control work.” Office of the Central Committee for Cybersecurity and Information Technology. http://www.gov.cn/xinwen/2020-02/10/content_5476711.htm.
- Kostka, Genia, and Sabrina Habich-Sobiegalla. 2021. “Covid-19 Contact Tracing Apps: Why They Are so Popular in China.” Merics. March 5, 2021. https://merics.org/en/short-analysis/covid-19-contact-tracing-apps-why-they-are-so-popular-china.
- Lew, L. (2021, November 14). “Coronavirus in China: tolerance wanes for Chengdu’s track and test regime.” South China Morning Post. https://www.scmp.com/news/china/science/article/3155959/coronavirus-china-tolerance-wanes-chengdus-track-and-test-regime.
- Zhu, Lin and Alfred M Wu, “Contact tracing: China’s health code offers some lessons.” (July 16, 2020). The Business Times Singapore. https://www.businesstimes.com.sg/opinion/contact-tracing-chinas-health-code-offers-some-lessons.
- People’s Daily Online — English. (2021, March 21). “China’s unified anti-epidemic digital health code used over 40 bln person-times.” People’s Daily Online — English. http://en.people.cn/n3/2021/0306/c90000-9825764.html.
- Chen, Shan, Tianjiao Liu, Xin Li, Yingjuan Luo, Li Xiao, Libing Zhang, Rongkang Wen, and Yonghong Lin. 2021. “Health QR Code Application in the Novel Containment Strategy and Healthcare Plan for Pregnant Women and Children Under Quarantine During the Summer Outbreak of SARS-CoV-2 Delta Variant in Chengdu, China: An Observational Study.” Risk Management and Healthcare Policy Volume 14 (November): 4499–4510. https://doi.org/10.2147/rmhp.s335803.
- O’Meara, Sarah. 2021. “China’s Data-Driven Dream to Overhaul Health Care.” Nature 598 (7879): S1–3. https://doi.org/10.1038/D41586-021-02694-1.
- Hinton, Geoffrey, Li Deng, Dong Yu, George Dahl, Abdel Rahman Mohamed, Navdeep Jaitly, Andrew Senior, et al. 2012. “Deep Neural Networks for Acoustic Modeling in Speech Recognition: The Shared Views of Four Research Groups.” IEEE Signal Processing Magazine 29 (6): 82–97. https://doi.org/10.1109/MSP.2012.2205597.
- LeCun, Yann, Yoshua Bengio, and Geoffrey Hinton. 2015. “Deep Learning.” Nature 521 (7553): 436–44. https://s3.us-east-2.amazonaws.com/hkg-website-assets/static/pages/files/DeepLearning.pdf.
- Krizhevsky, Alex, Ilya Sutskever, and Geoffrey E. Hinton. 2017. “ImageNet Classification with Deep Convolutional Neural Networks.” Communications of the ACM 60 (6): 84–90. https://doi.org/10.1145/3065386.
- Electronic Frontier Foundation. 2021. “AI Progress Measurement.” Electronic Frontier Foundation. 2021. https://www.eff.org/ai/metrics.
- Hassan, Hany, Anthony Aue, Chang Chen, Vishal Chowdhary, Jonathan Clark, Christian Federmann, Xuedong Huang, et al. 2018. “Achieving Human Parity on Automatic Chinese to English News Translation.” Microsoft Research. March 2018. https://www.microsoft.com/en-us/research/uploads/prod/2018/03/final-achieving-human.pdf.
- Lewis-Kraus, Gideon. 2016. “The Great A.I. Awakening — The New York Times.” New York Times. 2016. http://www.nytimes.com/2016/12/14/magazine/the-great-ai-awakening.html.
- Crumpler, William. 2020. “How Accurate Are Facial Recognition Systems — and Why Does It Matter?” Center for Strategic and International Studies. April 14, 2020. https://www.csis.org/blogs/technology-policy-blog/how-accurate-are-facial-recognition-systems-–-and-why-does-it-matter.
- Adjabi, Insaf, Abdeldjalil Ouahabi, Amir Benzaoui, and Abdelmalik Taleb-Ahmed. 2020. “Past, Present, and Future of Face Recognition: A Review.” Electronics 2020, Vol. 9, Page 1188 9 (8): 1188. https://doi.org/10.3390/ELECTRONICS9081188.
- Wikipedia Contributors. 2021. “AI Winter.” Wikipedia, The Free Encyclopedia. December 1, 2021. https://en.wikipedia.org/w/index.php?title=AI_winter&oldid=1052089413.
- Reese, Byron, and Andrew Ng. 2017. “Baidu’s Andrew Ng Talks AI with Gigaom.” Gigaom. January 11, 2017. https://gigaom.com/2017/01/11/baidus-andrew-ng-talks-ai-with-gigaom/.
- Roberts, Huw, Josh Cowls, Jessica Morley, Mariarosaria Taddeo, Vincent Wang, and Luciano Floridi. 2021. “The Chinese Approach to Artificial Intelligence: An Analysis of Policy, Ethics, and Regulation.” AI & Society 36 (1): 59–77. https://doi.org/10.1007/s00146-020-00992-2.
- China. State Council. (2015, July 4). “China unveils “Internet Plus” action plan to fuel growth.” China. State Council. http://english.www.gov.cn/policies/latest_releases/2015/07/04/content_281475140165588.htm.
- Justrecently. (2015, April 17). “A Chinese concept of Internet Revolution: a Need for Traditional Industries to be Reborn with New Bones.” Justrecently’s Weblog. https://justrecently.wordpress.com/2015/04/17/a-chinese-concept-of-internet-revolution-a-need-for-traditional-industries-to-be-reborn-with-new-bones/.
- Bekar, Clifford, Kenneth Carlaw, and Richard Lipsey. 2018. “General Purpose Technologies in Theory, Application and Controversy: A Review.” Journal of Evolutionary Economics 28 (5): 1005–33. https://doi.org/10.1007/s00191-017-0546-0.
- Wikipedia contributors. (2021, October 14). AlphaGo versus Ke Jie. Wikipedia, The Free Encyclopedia. https://en.wikipedia.org/wiki/AlphaGo_versus_Ke_Jie.
- Tsinghua University. 2018. “China AI Development Report 2018.” Tsinghua University. 2018. http://www.sppm.tsinghua.edu.cn/eWebEditor/UploadFile/China_AI_development_report_2018.pdf.
- Webster, G., Creemers, R., Triolo, P., & Kania, E. (2017, August 1). “Full Translation: China’s ‘New Generation Artificial Intelligence Development Plan’” (2017). New America. https://www.newamerica.org/cybersecurity-initiative/digichina/blog/full-translation-chinas-new-generation-artificial-intelligence-development-plan-2017/.
- Lee, Kai-Fu. AI Superpowers: China, Silicon Valley, and the New World Order (2018). Houghton Mifflin Harcourt.
- Silver, David, Julian Schrittwieser, Karen Simonyan, ioannis Antonoglou, Aja Huang, Arthur Guez, Thomas Hubert, et al. 2017. “Mastering the Game of Go without Human Knowledge.” Nature Publishing Group 550. https://doi.org/10.1038/nature24270.
- Hao, Karen. 2019. “We Analyzed 16,625 Papers to Figure out Where AI Is Headed Next.” MIT Technology Review. January 25, 2019. https://www.technologyreview.com/2019/01/25/1436/we-analyzed-16625-papers-to-figure-out-where-ai-is-headed-next/.
- Corbo, Jacomo, Oliver Fleming, and Nicolas Hohn. 2021. “Charting a Business Course for Reinforcement Learning.” McKinsey. 2021. https://www.mckinsey.com/business-functions/mckinsey-analytics/our-insights/its-time-for-businesses-to-chart-a-course-for-reinforcement-learning.
- Fatima, Samar, Gregory S. Dawson, Kevin C. Desouza, and James S. Denford. 2021. “Winners and Losers in the Fulfillment of National Artificial Intelligence Aspirations.” Brookings Institution. October 21, 2021. https://www.brookings.edu/blog/techtank/2021/10/21/winners-and-losers-in-the-fulfilment-of-national-artificial-intelligence-aspirations/.
- Budd, Jobie, Benjamin S. Miller, Erin M. Manning, Vasileios Lampos, Mengdie Zhuang, Michael Edelstein, Geraint Rees, et al. 2020. “Digital Technologies in the Public-Health Response to COVID-19.” Nature Medicine 26 (8): 1183–92. https://doi.org/10.1038/S41591-020-1011-4.
- Candelon, Francois, Matthieui Gombeaud, and Shervin Khodabandeh. 2021. “China’s Response to COVID Showed the World How to Make the Most of A.I.” Fortune. June 4, 2021. https://fortune.com/2021/06/04/covid-ai-china-artificial-intelligence-public-health-research/.
- For example, O’Meara cites the Go tournament in her reporting on China’s AI ambitions: “Then in 2017, the AI AlphaGo, developed by Google’s London-based company DeepMind, defeated the world’s number-one Go player Ke Jie — huge news in China, where the ancient board game is wildly popular. ‘This tiny storm became a typhoon and blew every scientist’s mind,’ says Xue [Yu Xue, a computer engineer and cell biologist at Huazhong University of Science and Technology in Wuhan]. ‘More and more scientists around me began to believe that AI could be useful in biomedical studies’” [81].
- Adamidi, Eleni S., Konstantinos Mitsis, and Konstantina S. Nikita. 2021. “Artificial Intelligence in Clinical Care amidst COVID-19 Pandemic: A Systematic Review.” Computational and Structural Biotechnology Journal 19 (January): 2833–50. https://doi.org/10.1016/J.CSBJ.2021.05.010.
- Zhao, Zhuo, Yangmyung Ma, Adeel Mushtaq, Abdul M Azam Rajper, Mahmoud Shehab, Annabel Heybourne, Wenzhan Song, Hongliang Ren, and Zion Tsz Ho Tse. 2021. “Applications of Robotics, Artificial Intelligence, and Digital Technologies During COVID-19: A Review.” Disaster Medicine and Public Health Preparedness, 1–11. https://doi.org/10.1017/dmp.2021.9.
- Gunasekeran, Dinesh Visva, Rachel Marjorie Wei Wen Tseng, Yih Chung Tham, and Tien Yin Wong. 2021. “Applications of Digital Health for Public Health Responses to COVID-19: A Systematic Scoping Review of Artificial Intelligence, Telehealth and Related Technologies.” Digital Medicine 4 (1): 1–6. https://doi.org/10.1038/s41746-021-00412-9.
- Wang, Lian, Yonggang Zhang, Dongguang Wang, Xiang Tong, Tao Liu, Shijie Zhang, Jizhen Huang, et al. 2021. “Artificial Intelligence for COVID-19: A Systematic Review.” Frontiers in Medicine (September): 1457. https://doi.org/10.3389/FMED.2021.704256.
- Kaushal, Karanvir, Phulan Sarma, S Rana, Bikash Medhi, and Manisha Naithani. 2020. “Emerging Role of Artificial Intelligence in Therapeutics for COVID-19: A Systematic Review.” Journal of Biomolecular Structure & Dynamics, 1–16. https://doi.org/10.1080/07391102.2020.1855250.
- Khan, Muzammil, Muhammad Taqi Mehran, Zeeshan Ul Haq, Zahid Ullah, Salman Raza Naqvi, Mehreen Ihsan, and Haider Abbass. 2021. “Applications of Artificial Intelligence in COVID-19 Pandemic: A Comprehensive Review.” Expert Systems with Applications 185 (December): 115695. https://doi.org/10.1016/J.ESWA.2021.115695.
- Abd-Alrazaq, Alaa, Mohannad Alajlani, Dari Alhuwail, Jens Schneider, Saif Al-Kuwari, Zubair Shah, Mounir Hamdi, and Mowafa Househ. 2020. “Artificial Intelligence in the Fight Against COVID-19: Scoping Review.” J Med Internet Res 2020;22(12):E20756 https://www.Jmir.Org/2020/12/E20756 22 (12): e20756. https://doi.org/10.2196/20756.
- Zhang, Daniel, Saurabh Mishra, Erik Brynjolfsson, John Etchemendy, Deep Ganguli, Barbara Grosz, Terah Lyons, et al. 2021. “Artificial Intelligence Index Report 2021.” AI Index Steering Committee, Human-Centered AI Institute, Stanford University. March 2021. https://aiindex.stanford.edu/report/.
- Dong, Jiancheng, Huiqun Wu, Dong Zhou, Kaixiang Li, Yuanpeng Zhang, Hanzhen Ji, Zhuang Tong, Shuai Lou, and Zhangsuo Liu. 2021. “Application of Big Data and Artificial Intelligence in COVID-19 Prevention, Diagnosis, Treatment and Management Decisions in China.” Journal of Medical Systems 45 (9). https://doi.org/10.1007/s10916-021-01757-0.
- Zhang, K., Liu, X., Shen, J., Li, Z., Sang, Y., Wu, X., Zha, Y., Liang, W., Wang, C., Wang, K., Ye, L., Gao, M., Zhou, Z., Li, L., Wang, J., Yang, Z., Cai, H., Xu, J., Yang, L., … Wang, G. (2020). Clinically Applicable AI System for Accurate Diagnosis, Quantitative Measurements, and Prognosis of COVID-19 Pneumonia Using Computed Tomography. Cell, 181(6), 1423–1433.e11. https://doi.org/10.1016/J.CELL.2020.04.045.
- Guerry, M., & Müller, C. (2021). World Robotics 2021: Presentation. International Federation of Robotics. https://ifr.org/downloads/press2018/2021_10_28_WR_PK_Presentation_long_version.pdf.
- Xinhua. (2021, January 18). “Across China: Chinese city uses robots to collect throat swab samples for COVID-19 testing.” Xinhua. http://www.xinhuanet.com/english/2021-01/18/c_139676901.htm.
- O’Meara, S. (2020). “Meet the engineer behind China’s first robot-run coronavirus ward.” Nature, 582(7813), S53. https://doi.org/10.1038/D41586-020-01794-8.
- Katz, L. (2020, March 14). “Coronavirus care at one hospital got totally taken over by robots.” 2020. https://www.cnet.com/news/coronavirus-care-at-one-hospital-got-taken-over-by-robots/.
- Global Times. (2021, November 4). “Robots ready for Beijing Winter Olympic Games to reduce contact amid the COVID-19 pandemic”. Global Times. https://www.globaltimes.cn/page/202111/1238089.shtml?id=11.
- Nan, Z. (2020, July 13). “Robots safeguard students’ health.” China Daily.
- Sani Pass. (2021, March 2). “How modern hospitals leverage mist disinfection gates for patient and healthcare workers safety?”. Sani Pass Blog. https://sanipass.net/how-modern-hospitals-leverage-mist-disinfection-gates-for-patient-and-healthcare-workers-safety/.
- Allen, D. (2021, November 15). “China: Flattening the Covid Curve.” MedicalExpo E-Magazine. https://emag.medicalexpo.com/china-flattening-the-covid-curve/.
- Shenzhen Daily. (2021, September 22). “Smart robots equip Nanshan quarantine hotel.” Shenzhen Daily.
- Sun, Y., Yang, Y., Yu, S., & Goh, B. (2021, September 27). “Pandemic pushes Chinese tech giants to roll out more courier robots.” Reuters. https://sg.news.yahoo.com/pandemic-pushes-chinese-tech-giants-150505046.html.
- iFlyTek. (2021, September 13). “iFLYTEK Reports 62% Increase in H1 2021 Net Profit.” PR Newswire. https://www.prnewswire.com/news-releases/iflytek-reports-62-increase-in-h1-2021-net-profit-301375517.html.
- Sun, T. Q., Ordás, T. G., Andrades, A. B., & Luis Calvo-Rolle, J. (2021). “Adopting Artificial Intelligence in Public Healthcare: The Effect of Social Power and Learning Algorithms.” International Journal of Environmental Research and Public Health 2021, Vol. 18, Page 12682, 18(23), 12682. https://doi.org/10.3390/IJERPH182312682.
- Sun, S., Xie, Z., Yu, K., Jiang, B., Zheng, S., & Pan, X. (2021). “COVID-19 and healthcare system in China: challenges and progression for a sustainable future.” Globalization and Health, 17(1), 1–8. https://doi.org/10.1186/S12992-021-00665-9/TABLES/1.
- Reuters. (2021, December 6). “Next pandemic could be more lethal than COVID, vaccine creator says.” Reuters. https://www.reuters.com/business/healthcare-pharmaceuticals/next-pandemic-could-be-more-lethal-than-covid-oxford-vaccine-creator-says-2021-12-06/.
- Lu, Q., Cai, Z., Chen, B., & Liu, T. (2020). “Social Policy Responses to the Covid-19 Crisis in China in 2020.” International Journal of Environmental Research and Public Health 2020, Vol. 17, Page 5896, 17(16), 5896. https://doi.org/10.3390/IJERPH17165896.
- Lazarus, J. v., Ratzan, S., Palayew, A., Billari, F. C., Binagwaho, A., Kimball, S., Larson, H. J., Melegaro, A., Rabin, K., White, T. M., & El-Mohandes, A. (2020). “COVID-SCORE: A global survey to assess public perceptions of government responses to COVID-19 (COVID-SCORE-10)”. PLoS One, 15(10 October), e0240011. https://doi.org/10.1371/journal.pone.0240011.
- Qingyi, Z. (2020, April 1). “Q31: Why is China able to practice closed-off community management?” Center for International Knowledge on Development. http://www.cikd.org/english/detail?leafid=213&docid=1320.
- Tian, W. (2021). “How China Managed the COVID-19 Pandemic.” Asian Economic Papers, 20(1), 75–101. https://doi.org/10.1162/ASEP_A_00800.
- Oka, T., Wei, W., & Zhu, D. (2021). The effect of human mobility restrictions on the COVID-19 transmission network in China. PLOS ONE, 16(7), e0254403. https://doi.org/10.1371/JOURNAL.PONE.0254403.
- Sobey, R. (2021, December 20). “Dr. Fauci predicts record-high number of coronavirus cases, slammed hospitals amid omicron variant: ‘A tough few weeks to months.’” The Mercury News. https://www.mercurynews.com/2021/12/20/fauci-predicts-record-high-number-of-coronavirus-cases-slammed-hospitals-amid-omicron-variant-a-tough-few-weeks-to-months/.
- The State Council is the chief administrative authority of the People’s Republic of China. See Wikipedia contributors. “State Council of the People’s Republic of China.” Wikipedia, The Free Encyclopedia. https://en.wikipedia.org/w/index.php?title=State_Council_of_the_People%27s_Republic_of_China&oldid=1059005992 (accessed December 20, 2021).
- Worobey, M. (2021). “Dissecting the early COVID-19 cases in Wuhan.” Science, 374(6572), 1202–1204. https://doi.org/10.1126/SCIENCE.ABM4454.
- Zimmer, C., Mueller, B., & Buckley, C. (2021, November 18). “First Known Covid Case Was Vendor at Wuhan Market, Scientist Says.” The New York Times. https://www.nytimes.com/2021/11/18/health/covid-wuhan-market-lab-leak.html.
- Schmidt, C. (2021, December 17). “Why Is Omicron So Contagious?” Scientific American. https://www.scientificamerican.com/article/why-is-omicron-so-contagious/.
- Sheperd, C., & Li, L. (2021, November 30). “As omicron variant spreads, China senses vindication over “zero covid” strategy.” The Washington Post. https://www.washingtonpost.com/world/asia_pacific/china-omicron-variant-coronavirus/2021/11/30/74e9788e-518d-11ec-83d2-d9dab0e23b7e_story.html.
- Statista. (2021, December 9). “COVID-19 tests by country.” Statista. https://www.statista.com/statistics/1028731/covid19-tests-select-countries-worldwide/.
- Wong, E., Barnes, J. E., & Kanno-Youngs, Z. (2020, September 17). “Local Officials in China Hid Coronavirus Dangers From Beijing, U.S. Agencies Find.” The New York Times. https://www.nytimes.com/2020/08/19/world/asia/china-coronavirus-beijing-trump.html.
- Crowley, M., Wong, E., & Jakes, L. (2020, March 22). “Coronavirus Drives the U.S. and China Deeper Into Global Power Struggle.” The New York Times. https://www.nytimes.com/2020/03/22/us/politics/coronavirus-us-china.html.
- Viala-Gaudefroy, J., & Lindaman, D. (2020). “Donald Trump’s ‘Chinese virus’: the politics of naming.” The Conversation.
- Zhou, L. (2020, June 23). “Trump’s use of “kung flu” is his latest effort to stoke xenophobia.” Vox. https://www.vox.com/2020/6/23/21300332/trump-coronavirus-racism-asian-americans.
- Subramaniam, T., & Hickey, C. (2020, September 16). “Timeline: Charting Trump’s public comments on Covid-19 vs. what he told Woodward in private.” CNN. https://www.cnn.com/interactive/2020/09/politics/coronavirus-trump-woodward-timeline/.
- Woodward, B. (2020). Rage. New York: Simon & Schuster.
- Wikipedia contributors, “Spanish flu,” Wikipedia, The Free Encyclopedia, https://en.wikipedia.org/w/index.php?title=Spanish_flu&oldid=1061359647 (accessed December 22, 2021).
- Kormann, C. (2021, October 12). “The Mysterious Case of the COVID-19 Lab-Leak Theory.” The New Yorker. https://www.newyorker.com/science/elements/the-mysterious-case-of-the-covid-19-lab-leak-theory.
- Capra, E., Godfrey, A., Loche, A., & Smith, J. (2021, May 17). “Innovation in viral-vector gene therapy: unlocking the promise.” McKinsey. https://www.mckinsey.com/industries/life-sciences/our-insights/gene-therapy-innovation-unlocking-the-promise-of-viral-vectors.
- Zhou, D., Song, H., Wang, J., Li, Z., Xu, S., Ji, X., Hou, X., & Xu, J. (2019). “Biosafety and biosecurity.” Journal of Biosafety and Biosecurity, 1(1), 15–18. https://doi.org/10.1016/J.JOBB.2019.01.001.
- Huang, H., Chen, Z., Shi, X., Wang, C., He, Z., Jin, H., Zhang, M., & Li, Z. (2021). “China in the eyes of news media: a case study under COVID-19 epidemic.” Frontiers of Information Technology & Electronic Engineering 2021 22:11, 22(11), 1443–1457. https://doi.org/10.1631/FITEE.2000689.
- Yang, J., & Wang, H. (2021). “Discursive Othering in the Fighting Against COVID-19: A Critical Discourse Analysis of the China Related Coverage of COVID-19.” 2020 International Conference on Language, Communication and Culture Studies, 31–35.
- Alshahrani, A. (2021). “A frame analysis of the language used by eight US media to describe the role of China and Chinese in spreading Covid-19 during late January to early June 2020.” Journal of Language and Linguistic Studies, 17(2), 1129–1140. www.jlls.org.
- Silver, L., Devlin, K., & Huang, C. (2020, October 6). “Unfavorable Views of China Reach Historic Highs in Many Countries.” Pew Research Center. https://www.pewresearch.org/global/2020/10/06/unfavorable-views-of-china-reach-historic-highs-in-many-countries/.
- South China Morning Post. (2020, August 20). “Wuhan pool party shows China’s ‘strategic victory’ over Covid-19, Beijing says.” South China Morning Post (YouTube). https://www.youtube.com/watch?v=MRuCv0yxpaA&t=16s.
- Skyscrapers & MegaProjects. (2020, February 1). “Official Timelapse of China’s Coronavirus Hospital Built in 7 Days.” Skyscrapers & MegaProjects (YouTube). https://www.youtube.com/watch?v=kaFUiUCbj-I&t=1s.